Untimely treatment of caries in children leads to the development of pulpitis - inflammation of tooth tissue, including blood vessels and nerve bundles. The lower molars are most often affected, but the disease occurs even on the anterior elements. Therefore, pulpitis in children occurs even more often than in adults. This is due to a number of factors:
- thin weak enamel;
- large volume of pulp;
- wide root canals;
- less mineralization;
- weak immunity.
In addition to caries, pulpitis can be caused by trauma, including poor treatment.
Symptoms
Inflammation occurs in acute and chronic forms. Acute occurs less frequently, but has more severe symptoms and occurs in two stages:
- serous. The inflamed pulp is filled with serous fluid. There are complaints of severe pain in the tooth, intensifying at night and when chewing. The pain, as a rule, is intermittent, appears once and subsides. Most often, the process occurs in teeth with unformed or absorbable roots. After 5–6 hours, a transition to another stage occurs;
- purulent. Pus forms in the tissues, which begins to melt cells and tissues. The severity of the condition is influenced by immunity, dental condition, and bacterial activity. If the pus has an outlet in the form of a carious cavity or fistula, then the pain is mild. In the absence of outflow, the pain syndrome is bright and long-lasting, intensifying when chewing or eating cold or hot food. The general condition may worsen and fever may appear.
Chronic pulpitis occurs after acute pulpitis or on its own and is characterized by vague symptoms. Pain can only occur under unfavorable factors - cold or hot, too sweet food. The child begins to chew on one side, an unpleasant odor appears, and a bursting and pressing sensation occurs.
The danger of this form is that it is almost asymptomatic. Because of this, inflammation affects more and more tissues. Chronic pulpitis is of three types:
- fibrous. The lightest and most common form. Fibrous tissue grows, the pulp may bleed, and episodic pain appears from mechanical and thermal contact;
- hypertrophic. Develops with severe destruction of the tooth crown. Pathological growth of pulp tissue occurs, which fills the carious cavity;
- gangrenous. The most severe form, accompanied by pulp necrosis. The tooth becomes gray and bad breath appears due to tissue decomposition.
Symptoms
If periodontitis is diagnosed in children, symptoms and treatment depend on the form of the disease (acute or chronic). In acute periodontitis, there is a sharp initial and severe, increasing and incessant pain. The intensity of pain increases when pressure is applied to the damaged tooth. Other signs include:
- The gums near the diseased chewing element swell noticeably.
- The child's body temperature rises.
- The appearance of weakness and attacks of nausea are noted.
- The lymph nodes become enlarged and pain is felt when pressing.
In case of chronic periodontitis, a child’s primary tooth, which is treated in a clinic, does not have characteristic signs. Painful sensations can occur if you press on a sore tooth, or during contact with hot or cold food. In addition, there are the following symptoms:
- A fistula forms on the gum if the disease develops into a granulating form.
- The child becomes drowsy, gets tired quickly, and general weakness appears.
- Appetite worsens.
- Increased body temperature.
How to recognize the problem and is emergency treatment required?
Due to the reduced sensitivity of the pulp, pain during inflammation may be mild and not cause severe discomfort. In this case, the process of tissue destruction occurs rapidly. It is important to visit the dentist regularly and not ignore your child’s complaints of pain when chewing or when eating cold and hot foods.
Treatment for pulpitis should be immediate. The disease is dangerous due to complications - periodontitis or periostitis. It can also spread to a permanent tooth that has not yet erupted and destroy it.
Preventive measures
Obviously, it is better to prevent a dental problem than to subject the child to treatment and, accordingly, stress. But for this it is necessary to take care of prevention, and for this purpose, parents should take note of the following recommendations:
- The sooner you start taking care of the condition of your child’s teeth and oral cavity, the better. Even during pregnancy, the expectant mother should eat properly and also enrich her diet with foods high in calcium and fluoride. At the same time, you should start carrying out daily hygiene procedures even before the first teeth appear - you can clean your gums from bacterial plaque using special napkins or fingertips,
The photo shows oral hygiene in a baby using a special napkin. - As soon as the child reaches the age when he can brush his teeth on his own, he needs to be taught daily hygiene. At the same time, he must learn how to clean correctly, and a pediatric dentist will help you with this,
The future smile depends on the health of baby teeth - You should limit your child’s consumption of sweets, including sweet mixtures for little ones. Excess sweets in the diet is one of the most common causes of dental caries in childhood.
- Regular preventive examinations at the dentist’s office will allow you to detect the problem in time, and therefore quickly deal with it. At the same time, it is better to show the baby to a specialist as soon as his first teeth appear.
Parents need to understand that treatment of baby teeth is an extremely important condition for the health of permanent teeth. Therefore, if caries or any other dental diseases develop, the child should be immediately shown to a specialist. And in order to prevent problems from arising, it is necessary to take your child to the dentist for preventive examinations 3-4 times a year.
Treatment methods
The treatment of primary teeth in general does not differ from the treatment of permanent elements. If the child’s condition is serious, there is a threat of infection spreading throughout the body, amputation is performed. In most cases, the tooth is preserved to prevent malocclusion. Therapy is carried out in different ways:
- traditional. Involves treatment in three visits. During the first one, the nerve is opened, a devitalizing paste with arsenic is applied for 24-48 hours or without it for a period of up to 7 days. On the second visit, a pulp mummification mixture based on resorcinol-formalin is placed into the canals. At the last visit, a permanent filling is installed;
- modern. It takes place in 1 – 2 visits. If the child can sit quietly for a long time at the doctor and the roots of the tooth are formed, extraction is performed. The nerve is removed either on the first visit or after applying the paste. Next, the canals are carefully processed, infected tissue is removed, an anti-inflammatory paste (for example, zinc eugenol) is applied and closed with a filling. The composition will gradually dissolve along with the roots when changing teeth;
- partial vital amputation. The doctor removes the upper portion of the nerve and applies an antiseptic and anti-inflammatory medication that seals the remaining living pulp.
When treating teeth with immature roots, a different approach is chosen. This is due to several reasons:
- the apex of the roots has not yet closed and there is a risk of infection of the permanent tooth germ;
- the roots are short and the channels are wide;
- trauma to the upper zone of the root can lead to disturbances in its formation;
- It is impossible to remove the entire pulp and perform a complete canal treatment.
Most often, they choose amputation of the pulp by any method or biological treatment, when the tooth is cleaned of the affected tissue and a paste with calcium hydroxide is applied for several days. After this, a filling is installed.
Pulpotomy of primary molars
In 1991, Yacobi et al wrote about the then-evolved techniques and materials for performing pulpotomy of primary molars. A year later, Croll and Killian described a technique for performing pulpotomy of primary molars using a mixture of zinc oxide powder and eugenol as a material to fill the pulp cavity. After performing a pulpotomy, the authors recommended covering the teeth with stainless steel metal crowns. This approach was modified from the original technique of Kaare Langeland, who described the toxicity of the use of formocresol in pulpotomy, and stated that the pulpotomy procedure itself was effective without the use of formocresol, and not because of it. If there is a need to achieve hemostasis, the author suggested using ferrous sulfate. Later, the use of zinc oxide eugenol (ZOE) for pulp capping and filling the pulp chamber space was reported to be successful. MTA is another alternative material that can be used for a similar purpose. MTA is a derivative of Portland cement and is currently most often used during pulpotomy.
A systematic review and meta-analysis by Lin et al found MTA to be the first choice material for pulpotomy of primary molars. In this article we will present three cases of pulpotomy of primary molars with their further covering with metal crowns. In one clinical case we performed the pulp cavity with COE, and in the other two with MTA.
Clinical case 1
A 39-month-old female patient and her mother sought advice regarding an acute carious lesion on the occlusal surface of a right lower second primary molar (Figure 1). The patient had already previously obtained an orthopantomogram, which was performed on the recommendation of the pediatric dentist (photo 2).
Photo 1. Occlusal caries of the lower second primary molar in a patient aged 39 months.
Photo 2. Orthopantomogram demonstrating an extensive cavity.
No other pathologies were found in the oral cavity. Their pediatric dentist recommended contacting a specialist to perform general anesthesia, perform a pulpotomy, and then cover the tooth with a metal crown. But at the appointment, the patient behaved absolutely adequately, was somewhat shy, but cooperated with the doctor, and based on this, it was decided to perform a pulpotomy under sedation with nitrous oxide, which was administered through a nasal mask. After the mother signed the informed consent, the patient was scheduled for the procedure the next day after the initial visit. During sedation, nitrous oxide was administered at a ratio of 20% nitric oxide/80% oxygen. The child also listened to music on headphones in order to avoid irritation from the sound of the drill. The area of the lower second molar was anesthetized by infiltrating a 4% solution of articaine hydrochloride with epinephrine in a ratio of 1:200,000. After the rubber dam was installed, access to the pulp was created using a cylindrical diamond bur (photo 3).
Photo 3. Exposure of the pulp chamber area.
During the formation of the access, it was confirmed that caries had penetrated into the area of the pulp chamber. After removal of carious dentin, the pulp tissue was removed to the orifice area using a sterile, low-speed No. 6 bur. Bleeding from the root canal area indicated that the pulp in these areas remained vital. A cotton ball soaked in water was placed over the orifice area and pressed, which allowed good hemostasis to be achieved without the use of ferrous sulfate solution or any other hemostatic agent (Figure 4). After this, the COE powder was mixed until it reached the consistency of a paste, and packed into the pulp chamber area, carefully removing the excess (photo 4).
Photo 4. COE-pulpotomy.
An orthodontic strip was placed around the tooth to stabilize the position of the rubber dam. The area where COE was applied was covered with modified glass ionomer cement, which was then polymerized and prepared for further fixation of the metal crown (photo 5). After 4 years and 8 months, the patient again sought help for the restoration of a permanent maxillary molar, in the area of which there were signs of carious lesions. During the examination, the successful result of the previously performed pulpotomy and crowning of the lower second primary molar was confirmed. However, given the level of root resorption, the degree of eruption of the second permanent premolar and the presence of minor inflammatory changes in the mucosa, it was decided to remove the primary molar under local anesthesia (photo 8).
Photo 5. View after preparation for a crown.
Photo 6. View 4 years and 8 months after the intervention.
Photo 7. Orthopantomogram 4 years and 8 months after the intervention.
Photo 8. View of the tooth after removal.
Clinical case 2
A 9-year-old boy was referred by his family dentist for treatment of an extensive carious lesion in the area of the right mandibular second molar (Figure 9). The area of the adjacent first primary molar was also noted to have caries, as was the area of the maxillary first primary molar. The radiograph showed signs of penetration of carious pathology into the pulp space (photo 10).
Photo 9. Caries of a primary molar in a 9-year-old patient.
Photo 10. X-ray showing an extensive carious cavity.
After obtaining informed consent from the parents, it was planned to perform a pulpotomy in the area of the lower second primary molar of the mandible on the left and perform a composite restoration in the area of the first primary molar. The patient contributed in every possible way to the intervention, and after anesthesia with a 4% solution of articaine hydrochloride with epinephrine 1:200,0000, a rubber dam was installed (photo 11). All further manipulations were performed similarly to those described in clinical case 1. Using a cylindrical bur, the cavity was cleared of caries (photo 12), the space of the pulp chamber was reached and hemostasis was ensured by means of sterile rollers, which were inserted into the pulp space under compression (photo 13-14). The dense MTA mixture (NeoMTA, NuSmile) was then packed using an amalgam condenser over the root canal orifices (Figure 15). Once the material had cured, the excess was removed with a cylindrical diamond bur, and preparation of the first molar began immediately for further restoration (Figure 16).
Photo 11. Insulation using rubber dam.
Photo 12. Removal of carious tissue.
Photo 13. Achieving hemostasis using cotton rolls.
Photo 14. View after achieving hemostasis.
Photo 15. Packaging MTA in the tooth cavity.
Photo 16. View after pulpotomy.
A bioactive composite (ACTIVA BioACTIVE-RESTORATIVE, Pulpdent) was introduced into the cavities of both teeth, after which it was photopolymerized (photo 17-18). After polymerization, a 5% fluoride varnish was applied to the mesial surface of the permanent first molar. When the contour of the restoration on the first primary molar was completely recreated, the rubber dam clamp was reinstalled on the permanent first molar and the preparation of the second primary molar for a metal crown began (photo 19-20). The latter was contoured, cut and polished according to the usual algorithm, after which it was fixed with modified glass ionomer cement. Excess cement was removed using a Hollenback instrument (Figure 21), and in the area of interproximal contacts - using dental floss. The maxillary first primary molar was restored at the next visit. Photographs and radiographs obtained 22 months after treatment are shown in Figures 22 and 23. After 22 months, the patient no longer returned for monitoring.
Photo 17. Filling the cavity with a bioactive composite.
Photo 18. Polymerization of a bioactive composite.
Photo 19. View after contouring the restoration in the area of the first primary molar.
Photo 20. View after preparing the tooth for a crown.
Photo 21. Removing excess cement.
Photo 22. View 22 months after treatment.
Photo 23. X-ray 22 months after treatment.
Clinical case 3
An 8-year-old boy was referred to the dentist due to the need for extraction of the second primary molar of the lower jaw on the left and restoration in the area of the first primary molar on the same side of the jaw (photo 24-25). Taking into account the initial parameters of the clinical situation, the child’s parents were offered a treatment option with a pulpotomy procedure and further covering with a metal crown. Using the same approach as Case 2, the pulp chamber space was completed with MTA in the orifice area, the tooth was then capped with a metal crown, and the first primary molar area was restored with a restoration (Figure 26). Hemostasis was achieved using sterile moistened cotton swabs, and the dental cavity was filled with a modified glass ionomer material over the MTA. 33 months after treatment, clinical examination and radiological monitoring data indicated a successful outcome of the intervention (photos 27-28). 33 months after treatment, both primary teeth of the lower jaw on the left side were also removed according to orthodontic indicators (photo 29).
Figure 24: An 8-year-old patient was referred for extraction of the mandibular left mandibular second primary molar.
Photo 25. X-ray of the patient before treatment.
Photo 26. View after pulpotomy.
Photo 27. View after 33 months.
Photo 28. X-ray after 33 months.
Photo 29. View of the tooth after extraction.
Discussion
The use of a rubber dam when performing pulpotomy of primary molars is one of the key factors to ensure the success of the manipulation. The rubber dam ensures both safety of the intervention and comfort during the procedure. In cases where the pulp is completely damaged, the pulp tissue shows almost no signs of bleeding, therefore, in such cases, it is necessary to perform a pulpectomy or consider the need for tooth extraction. In cases of extraction, it is necessary to remember the need to manufacture a retainer to replace the space, so as not to compromise the process of eruption of permanent teeth.
In the three clinical cases described above, we were able to achieve hemostasis using conventional cotton swabs without the use of any other additional means. In cases of heavy bleeding, sterile low-speed burs can be used to remove pulp from the orifice. You can also use cotton swabs soaked in a solution of ferrous sulfate, which should be placed into the cavity of the pulp chamber for 30-60 seconds. This procedure is often referred to as a “ferum sulfate pulpotomy,” although in fact this agent is only used to stop bleeding. It is more correct to call the manipulations as COE-pulpotomy or MTA-pulpotomy, depending on the material used to close the orifice area.
Authors: Theodore P. Croll, DDS Constance M. Killian, DMD Rachel L. Bresler, DMD
Is it possible not to treat pulpitis if the teeth are baby?
There is a common opinion that it is not necessary to treat baby teeth, because they will soon fall out. This is the biggest mistake parents make. Untreated pulpitis leads to irreparable consequences and even affects permanent teeth:
- purulent abscess, periodontitis, life-threatening condition;
- deep infection affecting the germ of a permanent tooth;
- malocclusion due to early tooth extraction due to untimely treatment;
- pain interferes with normal chewing of food, uneven load on the teeth leads to accelerated destruction of other elements.
What materials are used
Many parents are interested in what is currently used to fill children’s teeth. Not so long ago, the choice of materials used to fill children's teeth was not as diverse as it is today. At one time, dentists more often resorted to using amalgam, but this composition cannot be called completely safe and harmless to the body, especially when it comes to a child. Later they began to use glass ionomer cement, but it also has its disadvantages. For example, it takes quite a long time for the material to harden, which is not always convenient if there is a baby in the dental chair.
On a note! Often, special pastes are used to fill the root canals of baby teeth. Such compositions are not able to provide perfect tightness if used to fill a vertical cavity. In addition, after some time they dissolve, and therefore are not intended for permanent filling.
This is how a child’s teeth are filled with reflective composites.
To date, the situation has changed a little, and today pediatric dentists increasingly prefer fillings made of light-curing composite, as well as compositions that are a combination of a hybrid composite and glass ionomer cement. These materials are characterized by increased strength, are easy to polish and have a high degree of adhesion.
Prevention
The main method of preventing dental and oral diseases is regular visits to the dentist and treatment of caries in the early stages. It is important to teach a child hygiene and the rules of brushing teeth from the first years of life. Parents should control the diet, which should contain all the necessary substances, limit sweets and allow only water to drink at night.
Doctors at the VIMONTALE clinic treat pulpitis of primary teeth in children of any age. Specialists not only master modern painless techniques, but also know how to find contact with a child, know how to reduce anxiety and win the favor of the youngest patients.
Expert of the article you are reading:
Lozinskaya Alla Nikolaevna
Pediatric dentist, general dentist.
You may also be interested in:
Children's orthodontist Dental treatment for children Correction of bite in children Features of the treatment of childhood caries Removal of baby teeth Prevention of childhood caries Silvering of teeth in children
Show more
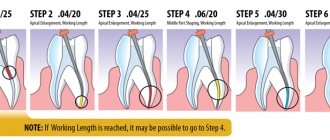
Features of machine treatment of dental canals in children
Regardless of the technique used, the dental specialist should consider the following points:
- Curved canals should be treated with a pre-curved tool.
- After removal, the reamers and files need to be cleaned and checked for damage.
- Rinsing the treated area should be done using an endodontic syringe equipped with a special needle.
Particular attention should be paid to medicinal treatment of the canals using EDTA and other drugs. It should be carried out at all stages of instrumental preparation, from the initial opening of the cavity to the final washing out before filling.
Our patients
Patient recommendations
Akhmedkhanov Said Rashidovich
Dental surgeon, general dentist, implantologist, orthopedic dentist, dental therapist.
Make an appointment 8 (499) 520-98-70
Make an appointment
Recommendations from patient Alekseeva O.V.
Akhmedkhanov Said Rashidovich
Dental surgeon, general dentist, implantologist, orthopedic dentist, dental therapist.
Make an appointment 8 (499) 520-98-70
Make an appointment
Recommendations from patient Zolotareva S.V.
Akhmedkhanov Said Rashidovich
Dental surgeon, general dentist, implantologist, orthopedic dentist, dental therapist.
Make an appointment 8 (499) 520-98-70
Make an appointment
Recommendations from patient Vera
Akhmedkhanov Said Rashidovich
Dental surgeon, general dentist, implantologist, orthopedic dentist, dental therapist.
Make an appointment 8 (499) 520-98-70
Make an appointment
Recommendations from patient Mikhail Ivanovich
Akhmedkhanov Said Rashidovich
Dental surgeon, general dentist, implantologist, orthopedic dentist, dental therapist.
Make an appointment 8 (499) 520-98-70
Make an appointment
Collapse
Reviews
Does your child have problems with their baby teeth? Do as our patients do - come to us for an appointment, and your baby’s teeth will be like new. At the Natadent clinic, treatment is quick, stress-free and without consequences for the child’s body.
Possible complications
If treatment for periodontitis in primary teeth is not started in a timely manner, the following consequences may occur:
- With an extensive inflammatory process, when more than one chewing element is affected, the rudiment of a permanent unit of the dentition can be severely damaged or completely destroyed.
- Considering the form of the disease, the process of resorption of the baby tooth root may accelerate. Or, on the contrary, a slowdown, which will provoke incorrect and untimely development and eruption of permanent chewing elements.
- Periostitis or osteomyelitis will develop.