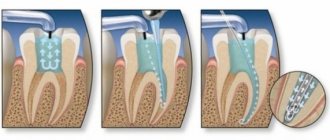
The result of dental canal treatment is the preservation and restoration of a tooth that is infected or has other pathology. The main task here remains cleaning the root canal. Infection and dying tissue must be removed from it. The resulting cavity is then securely filled. If treatment is not started in time, the inflammatory process will spread further and the tooth will have to be removed.
What is a root canal
In addition to enamel and dentin, any tooth has a fairly large internal cavity. Its main part is called the pulp chamber. Thin tubules extend from it. They are located along the entire length of the roots. These are root canals. The number of roots varies among different groups of teeth. Accordingly, the number of channels is also different. The front teeth have only 1 canal. Side groups can have from 2 to 4.
Dental tubules are narrow tubes with many branches. They originate at the top of the root. This place is called the apical foramen. From here, neurovascular tissue passes to each root. If it is inflamed or dead, it is removed during endodontic treatment. Next, the resulting cavity is cleaned of its residues, disinfected and sealed.
Obliteration of root canals. Clinical case.
A patient contacted us. The orthopantomogram image clearly shows complete obliteration of the lumen of the root canal of the 21st tooth.
Fig. 1 Complete obliteration of the root canal of the 21st tooth on an orthopantomogram
Diagnosis was made using cone beam computed tomography (CBCT).
Rice. 2 Sagittal section of the area of the 21st tooth on a CBCT image
Taking into account the skeletal asymmetry of the lower jaw in the image, the main cause of obliteration of the root canal in this case can be assumed to be trauma.
Rice. 3 Axial section of the upper jaw area with obliteration of the root canal of tooth 21
When is endodontic therapy needed?
Strict indications are required for dental canal treatment. After all, if the neurovascular tissue is removed, the tooth loses strength and becomes susceptible to destruction. Therefore, endodontic treatment should be carried out only in cases of inflammatory processes or traumatic injuries. The most common are:
- Pulpitis. This is an inflammation of the neurovascular tissue (pulp). It is a soft, fibrous substance. In addition to blood vessels and nerve endings, it includes connective tissue and lymphatic vessels.
- Periodontitis. Inflammatory process in the root and adjacent tissues.
These diseases have the following symptoms:
- Swelling of the gums and changes in its color, the appearance of fistulas and purulent formations on it.
- Acute pain in the tooth that is aching or throbbing. It gets worse at night or with pressure.
- Putrid odor from the mouth.
Sometimes these symptoms may be absent. In such cases, inflammation is determined only upon examination. Only a specialist can make a conclusion about the need for endodontic treatment. He selects the most effective treatment regimen depending on the situation.
Where is the tooth canal located, how is it structured
Human teeth have almost the same anatomical structure, including three main parts: crown, neck and root. Inside the tooth there is a pulp chamber, from which canals originate and extend all the way to the root. The pulp chamber contains the pulp or nerve of the tooth, which is a bundle of nerve fibers and blood vessels. Nerve fibers and vessels also pass through the entire internal space of the dental canal. The shape of the tooth canals can be either straight or curved, and their number varies depending on the type of tooth. Thus, the canines and incisors of the upper jaw have one canal, the canines and incisors of the lower jaw have two. There may be two or three canals in molars, and the maximum number of canals is observed in wisdom teeth - from three to five. The exact number of dental canals is determined using radiographic examination.
As mentioned above, the shape of the canals can have bends and turns, which complicates the process of their high-quality cleaning and treatment. Meanwhile, when treating canals, it is important to thoroughly clean their internal space - otherwise it will not be possible to stop the inflammatory process and save the diseased tooth.
Old methods of root canal treatment
Previously, endodontic treatment involved removing the pulp. For this purpose, for example, arsenic paste was used. It was inserted into the affected cavity and contributed to the death of the tissue. After this, the doctor removed the pulp from the tooth and filled it. This was the end of the treatment. Another common method was the placement of a resorcinol-formalin mixture. It froze in the cavity, thanks to which it was possible to stop the disintegration of tissues.
These methods had the following major disadvantages:
- Resorcinol-formalin and arsenic mixtures do not always completely kill the nerve. Therefore, when healing tissue, the patient could experience acute pain.
- Arsenic and resorcinol-formalin mixture are very toxic. They can accumulate in different organs.
- After pulp removal, tissue may remain in the root canals. Often they caused re-inflammation.
These methods of endodontic treatment were used due to the lack of adequate anesthesia, under which the affected pulp could be completely removed. Today dentistry has much more gentle methods.
Solving problems with very curved channels
The ultimate goal of endodontic treatment is to prevent the development of periapical lesions, as well as to create an environment conducive to their healing. To achieve such goals, it is necessary to adhere to certain classical principles of chemical disinfection and mechanical treatment of the root space. It is important to note that it is the success of the mechanical treatment of the endodontist that determines the effectiveness of all subsequent iatrogenic manipulations performed in the root canal.
For reliable obturation of the canal space with gutta-percha, it is necessary that it meet certain criteria, including:
- continuous conical shape of the main root canal, resembling a tapering funnel from the mouth to the apical foramen;
- narrowing of the cross-sectional diameter of the main canals in the apex area;
- preservation of the original shape of the channel during its processing;
- maintaining the original position of the apical foramen;
- maintaining the size of the apical foramen whenever possible.
The biological purpose of mechanical treatment of the endodontic space is as follows:
- restriction of the work of endodontic instruments within the boundaries of the root canal;
- prevention of extrusion of necrotic tissue into the postapical region;
- removal of all organic tissues from the space of the main and additional canals;
- creating a space of sufficient size to ensure effective irrigation and medicinal treatment without compromising the functional state of the tooth through excessive reduction in the thickness of dentin tissue.
Achieving the above goals in straight root canals is a fairly clear and logical process, however, in cases where there are various forms of anatomical variations in the endospace, this task becomes noticeably more complicated. It is especially difficult to achieve an adequate result of mechanical treatment of the canal in those with a pronounced bend of the endospace or in the presence of furcations and additional anastomoses (photo 1). It is quite difficult to follow classical intervention algorithms in such cases, therefore, to solve such problems, special NiTi files were developed, the sequence of application of which using the TCA technique helps to optimize the results of machining.
Photo 1a-c. Complex anatomical structure of root canals.
Treatment of canals with bends
Based on canal curvature, Nagy et al classified root canals into the following four categories:
- Straight or I-shaped (28% of root canals);
- Apically curved or J-shaped (23% of root canals);
- Curved along the entire length or C-shaped (33% of root canals);
- Multiple curved or S-shaped canals (16% of root canals).
Schäfer et al found that 84% of the root canals they studied were curved, while 17.5% had a second curvature and were classified as S-shaped. Of all the root canals with curves analyzed, 75% had a curvature level of less than 27°, 10% had a curvature ranged from 27 to 35°, and 15% had a pronounced curvature of more than 35°.
Traditionally, the severity of root canal curvature is described using the Schneider angle parameter: root canals with a bend of up to 5° are classified as straight canals, with a bend of 10 to 20° as moderately curved, and canals with a curve of more than 25° as severely curved. curved. Decades later, Pruett et al reported that two curved root canals can have the same Wein angle but completely different curvature parameters. To evaluate the latter, the radius of curvature parameter was introduced, which is defined as the radius of a circle passing through the curvilinear part of the channel. When using rotary tools, the number of cycles until the tool fails is significantly reduced as the radius of curvature decreases and the angle of curvature increases. Further attempts to mathematically describe the curvature of the channel on the basis of available two-dimensional radiographs led to the introduction into the theory of such parameters as the length of the curvature and its location, determined by the height and distance of the curvature. Estrela et al described a method for determining the radius of curvature of the root canal using CBCT slice data, which the scientists analyzed in specially developed software. According to their approach, the following three categories of root canal curvature were identified: small (r=4 mm), intermediate (r=4-8 mm) and large (r=8 mm). The smaller the radius of curvature, the greater its steepness. All of these attempts to describe root canal curvature had one goal: to develop an approach to assess the risk of apical foramen transportation and unexpected instrument separation.
Transport of channels and separation of instruments
According to the Glossary of Endodontic Terms, canal transport is the removal of the root canal wall structure on the outer side of the curvature in the apical half of the canal due to the properties of the files to restore their original linear shape. For stainless steel hand files and hand and machine NiTi files, the shape recovery properties are directly related to the size and taper of the tool. The larger the size and taper of the file, the more the file tries to restore its original shape, which is associated with an increase in the mass of metal in the structure of the tool. If the files exactly repeated the morphology of the endospace, then problems with transporting the canals would not arise at all, since in such an ideal situation the file would move strictly along the trajectory of the canal. Because the shape of the channels and instruments is different, each instrument moves along its own path within the curved channel, which is determined by its ability to recover. When attempting to increase the size of the apical foramen during mechanical treatment, as a rule, the amount of reduction of dentin tissue on the outer apical part of the curvature increases. To prevent this effect, doctors try to use instruments of a larger cone, but of a smaller size, for mechanical processing of the apical space in canals with pronounced curvature. Increasing the cone with this approach leads to a reduction in the angle of the bend, a decrease in its length and an increase in the radius with a reposition of the bend more apically (photo 2).
Photo 2. Treatment of the endospace leads to changes in bending parameters.
Reducing the volume of treatment of the apical part of the canal in those with pronounced curvature is indicated with the need to achieve the following goals:
- a smaller preparation diameter is associated with a smaller volume of canal wall reduction, a smaller increase in file size, and therefore with a lower risk of developing undesirable effects;
- files of smaller diameter are characterized by greater elasticity and less resistance to fatigue, thus, when working with these files, the possibility of transporting the canal as the size of the apical foramen increases is reduced.
The above-mentioned approaches to instrumental treatment of root canals, although safer, are also characterized by a number of disadvantages. Firstly, an increase in the taper of the endospace in its coronal part to ensure easier patency in the apical third provokes excessive reduction of dentin tissue, which compromises the biomechanical prognosis of the tooth. In addition, processing canals with smaller files makes it difficult for irrigation solutions to penetrate to the appropriate depth of the endospace. In canals with pronounced bends, the possibility of adequate irrigation of the root canal directly depends on the possibility of sufficient instrumental expansion of the apical third. Apical preparation of the apical part of the canal in order to achieve the appropriate level of disinfection in conditions of pronounced curvature is one of the most difficult practical tasks in endodontics, especially considering the prevalence of modern principles of minimally invasive interventions. In addition, there is a high risk of separation of rotary mechanical files in canals with pronounced curvature. The causes of such complications can be two main mechanisms: cyclic fatigue and torsion fatigue. When a rotary tool is activated within a curved channel, constant tensile and compressive stresses are generated within the physical center of rotation of the curvature. If the tip of the file is blocked in the endospace structure and the motor continues to rotate, the shear moment of the tool material exceeds its limit values, which also leads to the development of maximum levels of torsional fatigue (torsional fatigue). The greater the complexity of the morphology of channel bends, the fewer cycles of operation under such conditions the instrument can withstand.
Using Shape Memory Controlled Files
NiTi alloys are softer than stainless steel, but have a lower level of elasticity (about one-fourth to one-fifth that of stainless steel). At the same time, this material is more durable, rigid and elastic, due to which NiTi files are characterized by shape memory. NiTi files used in endodontics contain approximately 56% nickel and 44% titanium. However, they can exist in the form of two different temperature-dependent crystal structures called martensite (low-temperature phase) and austenite (high-temperature phase). The lattice organization can be transformed from austenitic to martensitic state by controlling temperature and stress. During the reverse transformation, the alloy passes through an unstable intermediate crystallographic phase called the R phase. The use of files during endodontic treatment provokes the development of stress, which, in turn, causes an instantaneous martensitic transformation of the NiTi file. A change in the shape of a tool is associated with a change in the parameters of its volume density. It is this property of the file, which is the ability to withstand stress without developing permanent deformation, that is called superelasticity. Superelasticity is most pronounced at the beginning of stress development, when the tool can easily overcome up to 8% deformation. After 100 deformations, this level drops to 6%, and after 100,000 – to 4%. It is within these boundaries that the shape memory effect is observed. In addition to stress, martensitic transformation of a file can also be caused by temperature changes. When the austenitic phase of a NiTi file cools, it begins to transform into martensitic phase. The temperature at which the martensite phase is completely restored again is called the temperature of the final transformation of martensite. When the martensite phase is heated, it begins to transform into the austenite phase. The temperature at which this phenomenon begins is called the temperature at which the austenite phase begins. At the final transformation temperature of austenite and above (Af), the material completes its shape memory transformation and demonstrates its superelastic properties. Until 2011, the Af temperature for most available NiTi tools was at or below room temperature. As a result, during clinical use, conventional NiTi files were in the austenitic phase, exhibiting their shape memory and superelasticity properties. In 2011, COLTENE introduced controlled shape memory files (CSF). The production of these tools involves the implementation of a unique thermomechanical process that controls the memory of the material, providing special elasticity and durability of the files, which is not typical for all other types of NiTi analogues. The Af-transformation temperature of CPF files is clearly higher than body temperature, as a result of which these files are in the martensite stage during operation in the endospace. In this phase, the instruments remain soft, plastic, without shape memory, and can be easily deformed, but after that they restore their shape and original elastic properties when heated to temperature Af.
A hybrid martensitic microstructure, like that used in HyFlex CM (COLTENE) files, also has a higher level of strength than an austenitic microstructure. At the same stress intensity, the rate of crack propagation in the structure of the austenitic phase is much higher than in the martensitic phase. A quantitative model for studying the process of crack development in the file structure made it possible to establish that the martensitic transformation of NiTi files increases the fracture strength of the tool by 47%.
More recently, the thermomechanical processing mechanism of CM has been combined with the mechanical fabrication procedure of NiTi files. Thanks to electrical discharge machining (EDM), it was possible to increase the surface hardness of files, their cutting efficiency and achieve unique parameters of resistance to functional fatigue. In the first published paper that demonstrated the results of using these files, the surface of the instruments was described as typical after an intrinsically safe specific treatment, and the level of degradation remained quite low even after multiple endodontic procedures. The authors also found that these files have surprisingly high levels of resistance to cyclic fatigue, and have a high safety profile even when working in highly curved canals, which has been confirmed in laboratory conditions. Pedulla et al also reported higher fatigue resistance values for HyFlex EDM (COLTENE) files, even compared to reciprocating machining and M-wire files.
Unfortunately, the literature data concerning the study of flexural stiffness and fracture resistance during the development of cyclic fatigue were carried out on NiTi files at room temperature. However, room temperature is not clinically significant. The use of modern instruments takes place at body temperature, which automatically excludes the possibility of direct application of the findings of previous studies in clinical practice. It is apparent that the transformation temperature (Af) of NiTi files designed for rotary or reciprocating processing can influence their clinical behavior under normal human body temperature conditions. Hulsmann et al (2019) reported that ambient temperature has a 500% influence on the service life of endodontic instruments. If the transformation temperature approaches body temperature, this can cause tools to appear flexible and fatigue resistant, but in fact become more rigid and less fatigue resistant. The Af of HyFlex EDM files was found to be close to 52°C, which is much higher than body temperature. Temperature analysis of EDM files confirmed the presence of a monoclinic structure of B19 martensite and a rhombohedral R phase. Thus, EDM instruments are always in the rhombohedral R-phase and martensitic crystallographic state at clinically relevant temperatures during endodontic treatment. The martensitic structure at body temperature allows these files to have excellent flexibility and resistance to fracture, as well as the absence of restoring forces, making them ideal for use during the machining of curved or morphologically complex canals.
Sequence of using HyFlex EDM Max files when processing curved canals
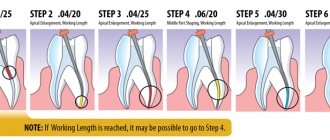
EDM technology has made it possible to implement the principle of endodontic expansion with a single rotary file. Generally, in most clinical cases, a 25/~ HyFlex EDM OneFile can be used with short peck movements while being sure to keep the instrument edges clear of debris and provide adequate irrigation. The OneFile is characterized by a size of 25 with a taper of 0.08. In this case, the taper of 0.08 is constant in the upper apical 4 mm of the instrument, but gradually decreases to 0.04 in the coronal part of the instrument. The file is characterized by the presence of three different cross-sectional zones along the entire length of the working part (rectangular in the apical part and two different trapezoidal cross-sections in the middle and coronal parts of the instrument). Thus, the developers managed to increase the file’s resistance to destruction and its cutting efficiency. When wider apical preparation is required, the designer introduces the following three HyFlex EDM finishing files with constant taper (40/.04, 50/.03 and 60/.02). For narrowed and obliterated canals, as well as for thin, long and S-shaped canals and canals with more than a 27° bend and a radius of curvature of less than 5 mm, a single file protocol is not indicated. In such cases, it is necessary to combine tools in order to achieve the most predictable treatment result. This is why the developer has also provided the Max Curve HyFlex EDM tool sequence, which includes files 15/.03, 10/.05 and 20/.05. The use of these files allows us to minimize the process of increasing the taper of the endospace, thus ensuring the minimum possible reduction of dentin on the canal walls. The Max Curve HyFlex EDM tool sequence can be used with the tactile controlled activation technique. Once the canal is identified, the minimal carpet is recreated using a 10/.02 stainless steel hand file. The 15/.03 HyFlex EDM tool is then used to follow the path of the carpet. After this, the 10/.05 HyFlex EDM file is used to widen the middle part of the canal. The apical 3 mm of the 10/.05 file act as a guide tip (without adhesion to the canal walls, photo 3). File 20/.05 HyFlex EDM is used as a final file to achieve the final smooth shape of the canal. After expansion with a 20/.05 instrument, the canal can be obturated with a 20/.05 gutta-percha cone and GuttaFlow biothermal sealer (COLTENE). The file sequence is easy to remember and ensures efficient and safe treatment of the endospace even in the most difficult clinical situations.
Photo 3. Sequence of HyFlex EDM Max Curve files.
Tactile control activation
In order to minimize the approach of using files with increasing taper, a tactile-controlled activation technique was proposed (photo 4a). This mechanical endospace technique can be defined as activating the stationary file only after it has been completely inserted into the patent canal. Essentially, the activation of the file occurs after the tactile sensation of achieving maximum adhesion of the cutting grooves to the walls of the endospace. Passive (non-activated) application of files is also useful, especially in cases of limited oral opening and incomplete visualization of the working field. Tactile-controlled activation can be classified into that during tool movement and during tool withdrawal. After creating access to the pulp cavity and localizing the mouths of the canals, their patency is ensured by the 10/.02 instrument. After this, the 15/.03 file is installed in the tip and inserted into the endospace until maximum resistance is felt (point A, photo 4b).
The file is then activated and pushed in the apical direction until the activated file reaches the point of resistance (point B, Fig. 4c). After this, the file is removed from the channel. The cutting edges of the instrument are cleared of debris, checked for deformations, and irrigation of the endospace is provided. The second time the same file is introduced, which can now go deeper in a passive state (point B, photo 4d). Re-activating the file will allow the file to advance the required length closer to the apical foramen (point C, photo 4e–g). Work with this tool is stopped only after it reaches the working length (point D, photo 4h). After reaching the working length, begin using the second file in the Max Curve sequence according to the protocol described above.
Photo 4a-h. Tactile controlled activation.
The thin apical 2 mm of a 10/.05 file will always remain free within the canal, which guides the file along the path of the endospace anatomy without the risk of developing excessive retention and breakage. File 20/.05 will ensure the final formation of the endospace and the conditions to ensure its proper disinfection and obturation. Mechanical processing of wider apical openings is achieved by increasing the width of the instruments used in particularly complex canals, such as those shown in photos 5 and 6; The use of a 20/.05 file would be most indicated, given the need to achieve proper disinfection of the endospace and minimize the risk of instrument separation. The TKA technique aims to minimize the time it takes to expand the endospace with an activated file, using file activation only when necessary to advance the instrument. With this approach and through the use of HyFlex EDM Max Curve files in a sequential manner, most anatomical variations of root canals can be treated without compromising the safety profile of the procedure.
Photo 5a-g. Treatment of the S-shaped mesiobuccal canal of the maxillary second molar using HyFlex EDM Max Curve files using the TKA technique: a) pre-treatment radiograph; b) radiograph after treatment; c) formation of the access cavity; d) view after processing with HyFlex EDM 15/.03 file; f) processing with HyFlex EDM 20/.05 file; f) obturation with gutta-percha pins 20/.05; g) view after obturation.
Photo 6a-d. Treatment of the S-shaped mesial canal of the mandibular second molar using HyFlex EDM Max Curve files: a) visualization of deep carious lesions; b) view after processing with HyFlex EDM 15/.03 file; c) view after obturation; d) view after restoration.
conclusions
NiTi files with CM effect are extremely flexible and have excellent fatigue resistance. They can be activated within the canal and passively moved along the bending path, guided by the original anatomy of the endospace. The TKA technique allows minimizing the time of close interaction of files with root dentin. During mechanical processing of the endospace, constant feedback tactile control of the manipulation is provided. For particularly complex clinical cases, a special sequence of HyFlex EDM Max Curve files has been developed, allowing clinicians to stay in tune with constantly moving progress.
Author: Dr Antonis Chaniotis (Greece)
Modern methods of endodontic treatment
In the treatment of tooth canals today there are two approaches: therapeutic and surgical. Let's look at them in more detail:
Therapeutic treatment. With this method, it is possible to preserve the entire pulp or at least part. The drug is placed into the cavity. The pulp chamber is isolated using a special gasket, then the tooth is filled. The drug can also reach tissues through dentin. To do this, special bandages with antibiotics are applied to the tooth. This therapy is used only in the initial stages of the inflammatory process.
Surgery. In this case, the pulp is completely removed, the canals are cleaned, disinfected and sealed. There are the following methods for filling cavities:
- Classical. The canals are filled with conventional filling material.
- Vertical filling. A special filling composition is administered as an injection.
- The use of thermophiles. A special heated composition on a carrier is placed into the cavity.
Sometimes, in order to cure the canal, you have to remove the tip of the root. This measure is necessary for cysts, granulomas, perforations, fibroids and other problems.
Modern methods of treatment
Highly qualified and experienced specialists at the Dentpremium Dentistry Center use exclusively modern methods of treating inflamed tooth canals.
- Therapeutic or biological. This method allows you to save part of the fabric or the entire remote control. The biological method is effective only at the initial stage of the disease. Treatment consists of placing an anti-inflammatory drug into the pulp chamber with a temporary filling, or applying antibiotic dressings to allow the drug to flow through the dentin.
- Pulp extirpation. Treatment involves removing absolutely all neurovascular tissue, cleaning the cavity, treating with antiseptics and sealing. For treatment, filling, injection of gutta-percha (thermoplasticized) or filling with thermophiles are used.
In the most severe cases, when there is a cyst, granuloma or other formation, resection of the root apex is performed.
Stages of endodontic treatment
- Diagnostics. If there is a suspicion of problems in the dental canal, an x-ray is taken. The specialist can also study the images that the patient already has. Depending on the diagnostic indications, treatment is selected.
- Pulp removal. First, the dentist anesthetizes the tooth. Then he opens it and removes all damaged tissue. Next, the cavity is given a convenient shape. Then the channels are disinfected using a special solution.
- Root canal filling. The cavities are filled with special materials. They are divided into hard (pins), hardening (various cements) and plastic (paste or gutta-percha). The most modern are the latter.
- Tooth restoration. This is the restoration of the shape of a tooth using a filling, crown or inlay.
Diagnostics
Treatment of impassable root canals begins with determining their length and anatomical features. The most informative diagnostic method is radiography. To obtain accurate data on the condition of the tissues, a photograph of the tooth root is taken with the instrument inserted into it. This allows you to see:
- length of root canals,
- the presence of curvatures and perforations,
- impassable areas.
The condition of the periodontium is also assessed. This allows you to determine further treatment tactics.
Canal treatment using a microscope
The diameter of the root canal of a tooth is approximately 1 millimeter. In such conditions it is impossible to work with it without special optics. The dental microscope allows you to increase visibility up to 32 times. Therefore, it is increasingly used in modern dentistry.
Advantages of using a dental microscope:
- The specialist can see and remove only tissues affected by inflammation, without touching healthy ones.
- An excellent overview of the tubule orifices is achieved. Seeing the number of their branches, depth and directions is very important during endodontic treatment.
- Due to targeted treatment of the pulp, complications can be avoided. The possibility of perforations is also eliminated.
Recommendations after endodontic treatment
After stopping the inflammation of the pulp, it is necessary to consolidate the result. To do this, the patient must adhere to the following simple rules:
- Do not eat spicy, cold or hot food for several days. You need to wait until the treated teeth lose sensitivity.
- Maintain oral hygiene. You need to brush your teeth and floss twice a day.
- Eliminate solid foods from your diet for a while. Failure to comply with this rule can lead to tooth decay.
- Go to the dentist for dental checkups 2 times a year.
After endodontic treatment, teeth will become especially sensitive. This is how the body reacts to the filling material. However, after a few days this effect will disappear.
Cost of services
Treatment of dental canals Price
Treatment of dental canals from 3000 rub.
1-canal tooth (mechanical and medicinal treatment of the canal) 900 rub.
1-canal tooth (canal filling with gutta-percha pins) 750 rub.
2-canal tooth (mechanical and medicinal treatment of canals) RUB 1,500.
2-canal tooth (canal filling with gutta-percha pins) 980 rub.
3-canal tooth (mechanical and medicinal treatment of canals) RUB 2,100.
3-channel tooth (canal filling with gutta-percha pins) RUB 1,300.
Expert of the article you are reading:
Akhmedkhanov Said Rashidovich
Dental surgeon, general dentist, implantologist, orthopedic dentist, dental therapist.
You may also be interested in:
Dental treatment during pregnancy Dental consultation Treatment of dental cysts Increased sensitivity of teeth: causes and methods of treatment Filling of dental canals Treatment of pulpitis Treatment of fistula on the gums Treatment of flux (periostitis)
Show more
Cost of treatment
Dentistry Dentpremium is a center of expert medicine that provides professional services at affordable prices. For dental canal treatment, the cost is calculated taking into account several factors: the number of root canals, the method and materials used, the total volume and complexity of the specialist’s work.
On the clinic’s website you can see the price list, which indicates the average cost of root canal treatment. After an examination in the dentist’s office and receipt of diagnostic results, the attending physician will be able to announce what the final cost for root canal treatment will be.
On the website of the Dentpremium clinic you can find all the information you are interested in, make an appointment or a free consultation, and also read reviews about root canal treatment in our center. If you have any questions, you can contact us by phone.