Current problem
For most people, heartburn is simply an occasional discomfort. Approximately 20% of the population of highly developed countries experience it at least once a month.
But for the 6% of people who have a chronic form of heartburn known as gastroesophageal reflux disease (GERD), unresolved (untreated) symptoms can lead to various health complications. People with erosions in the lining of the esophagus due to acid reflux often do not realize the harm of GERD until they have advanced stages of the disease.
If you experience frequent or prolonged heartburn (twice a week on a regular basis), consult your doctor. Here are nine reasons why you shouldn't ignore the symptoms of gastroesophageal reflux disease.
What to do?
If the color of saliva changes, it is best to consult a general practitioner. If necessary, he will refer the patient to other specialists. At home, without consulting a doctor, you can only cope with some of the causes of changes in the color of saliva. Of course, the easiest way to improve oral hygiene is to brush your teeth twice a day, use dental floss and mouthwash. You can also treat gingivitis at home in the early stages of development:
- Use special toothpastes with herbal ingredients, as well as similar rinses.
- Regularly rinse the mouth with antiseptic and anti-inflammatory solutions, for example, Miramistin, infusion of chamomile and calendula, etc.
- Adhere to a proper and balanced diet, do not injure inflamed gums with hard food.
If discomfort and redness do not go away within 2-3 days, you need to seek help from a dentist. In such a situation, targeted treatment may be required, including taking antibiotics and other medications.
Development of inflammation in the esophagus (esophagitis)
In gastroesophageal reflux disease, food, acid, and digestive juices back up into the esophagus. Over time, this causes irritation and swelling of the mucous membrane lining the inside of the esophagus. This is esophagitis. If acid exposure in the esophagus is observed for just a few weeks, then inflammation of the mucous membrane can already develop. This can cause discomfort and even pain along the midline of the abdominal wall, “in the pit of the stomach,” where the right and left ribs meet at the sternum. This inflammation makes the esophagus vulnerable to even more dangerous conditions - erosions or scars.
What diseases appear in the mouth in the morning?
Some gum diseases can cause saliva to turn brownish. Most often, such symptoms are observed with gingivitis and periodontitis - an inflammatory process in such areas of the oral cavity. A small amount of blood is released from the affected gums, which accumulates in the mouth overnight and oxidizes, changing the color of the saliva. In addition, such diseases can make themselves felt through pain, discomfort when eating solid foods, and bleeding during daily brushing of teeth.
Treatment of gum diseases is carried out under the supervision of a dentist. Sometimes it is possible to cope with an unexpressed inflammatory process on your own - with the help of regular rinsing and proper oral care.
Esophageal stricture
If esophagitis continues for too long, the resulting scar tissue can narrow the esophagus. This stricture can lead to difficulty passing and swallowing food, which can become stuck at the level of scar tissue, causing pain.
Large pieces of food may become stuck and this situation may require endoscopic intervention to remove them. The stricture may cause frequent choking when eating. Because of this, patients often refuse to eat and lose a lot of weight.
Stricture is treated by widening or stretching the esophagus (bougienage or dilatation). These treatment procedures can have multiple effects on the stricture. But taking stomach acid blockers (proton pump inhibitors, PPIs, or H2 blockers) may prevent scarring in the esophagus from returning in the future.
Why does drool turn dark due to natural factors?
A change in the color of saliva towards brown can be explained quite simply - by the lack of proper oral hygiene in the evening. If you eat food with coloring properties in the evening, its particles may remain in the interdental spaces. Overnight, saliva will dissolve them, and in the morning its color will be completely unusual.
Sometimes food fragments get stuck in dentures, dental appliances (plates or braces), cavities, etc.
Most often, saliva changes color under the influence of chocolate and sweets, but rye bread and other food products can also be the culprit for such changes.
Throat and voice problems
The main symptom of gastroesophageal reflux disease is heartburn, but not all people feel or report it. They may have other symptoms that are more difficult to diagnose. Doctors call these cases "silent reflux," or asymptomatic reflux. The patient may not have heartburn as classically described in textbooks, but they may have various other problems that occur outside the esophagus, such as hoarseness, voice changes, sore throat, or chronic cough. They feel as if there is a lump or hair in their throat and constantly have to clear their throat by coughing and clearing their throat.
Tumor formations
Cancerous tumors can be localized in different parts of the human body, including the throat, esophagus and tongue. In some cases, such neoplasms become ulcers capable of releasing exudate. In such a situation, the patient’s saliva may acquire an atypical color, for example, turn brown. However, in this case, cancer makes itself known by other signs, for example, the sensation of a foreign body or visually noticeable changes in the mucous membranes.
Breathing problems
If stomach acid accidentally flows into the windpipe after gastroesophageal reflux disease causes it to enter the esophagus, GERD can worsen asthma or pneumonia. Even without lung problems, GERD can cause shortness of breath and difficulty breathing. And treatment in this situation can be a double-edged sword. Because GERD medications, such as proton pump inhibitors, may actually increase the risk of pneumonia. (They can promote bacterial growth and suppress coughing, which is designed to help clear the lungs.)
Pay your doctor's attention to your lung function when treating reflux.
Is prevention possible?
Prevention is possible and it is available to everyone:
- You need to give up fatty foods.
- The diet must include fruits and vegetables.
- You should drink up to 2 liters of clean water per day.
- If you also experience dry mouth, you can suck on lollipops, mints, or chew gum for about three minutes to increase saliva production. They should not contain sugar.
- You should stop smoking and drink a minimum amount of alcohol.
- Use a quality mouthwash regularly.
To avoid this problem, you should think about your lifestyle in advance. You should not test your health with bad habits, you need to eat proper and healthy food. It is also important to contact your dentist and other doctors in a timely manner. If colds or other diseases appear, you need to treat them.
Esophageal ulcers
Stomach acid can erode the lining of the esophagus, causing sores and ulcers. Esophageal ulcers are different from stomach ulcers, which are usually caused by bacteria. People with wounds and sores may spit up blood and may also vomit blood. They may see blood in their stool. The blood may be red, cherry red, or like coffee particles. In stool, blood from the esophagus and stomach usually turns black when passing through the small intestine, the color and appearance of oil - viscous, slippery, and difficult to wash off.
Contact your doctor immediately if you have these symptoms. Endoscopy can detect ulcers of the esophagus. Acid-blocking or acid-lowering medications may make them disappear.
Diagnostics
If yellow sputum is present, the patient requires the help of a general practitioner or pulmonologist. During a physical examination of the patient, attention is paid to the participation of the chest in breathing, retraction of the intercostal spaces, and local areas of pain on palpation. Auscultation of the lungs provides valuable information - a preliminary diagnosis is made based on the presence of wheezing, harsh or amphoric breathing. The diagnostic scheme includes the following methods:
- X-ray studies.
On a survey X-ray of the chest in two projections, you can see areas of infiltration in the lungs, a round shadow with a horizontal fluid level, and local compaction. To diagnose tumors, a CT scan of the chest is performed. To confirm chronic bronchitis, bronchography is performed. - Endoscopy of the bronchial tree.
Bronchoscopy with visual examination of large and medium-sized bronchi is an informative method for diagnosing chronic inflammatory and fibrotic processes and detecting malignant tumors. During the examination, biopsies of suspicious tissue areas are taken for examination under a microscope. - Functional techniques.
In chronic diseases of the bronchopulmonary system, external respiration is impaired. To detect pathology, spirometry is prescribed, with the help of which the forced expiratory volume, vital capacity of the lungs, and other indicators are assessed. For express research, peak flowmetry is indicated. - Sputum tests.
The cytological method is aimed at identifying eosinophils and neutrophils, specific crystals and spirals of mucin in the tracheobronchial secretion. Culture with an antibiogram is used to determine the type of bacterial pathogen that caused the disease.
Additional diagnostic methods include a hemogram, which determines leukocytosis with an increase in ESR, eosinophilia, lymphopenia, as well as a biochemical blood test, which determines acute phase indicators and the ratio of plasma proteins. In chronic bronchopulmonary processes, heart function is often disrupted, so the examination plan includes an ECG and EchoCG.
Sputum analysis
Barrett's esophagus
If left untreated for many years, persistent acid reflux can form changes in cells known as Barrett's esophagus, which is considered a precancerous condition. This condition does not cause many symptoms other than those of reflux. A doctor can diagnose it by performing an endoscopy.
If you have heartburn more than twice a week for a long time, or if you have symptoms of gastroesophageal reflux disease that are getting worse or you have discovered new ones that you didn't have before, these are all reasons to get checked and have an endoscopy.
Reasons for color changes in the morning
In fact, there are quite a few factors that can change the color of saliva. Among them are:
- Quite natural reasons.
- Otolaryngological diseases.
- Malfunctions of the gallbladder.
- Diseases of the digestive tract.
- Some problems in the condition of the oral cavity.
- Tumor formations.
It can be quite difficult to independently identify the cause of dark saliva in your mouth. If such a condition is in no way related to natural factors, it is necessary to seek medical help to undergo an examination and make a correct diagnosis.
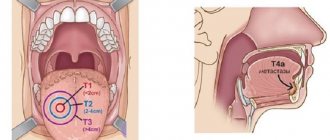
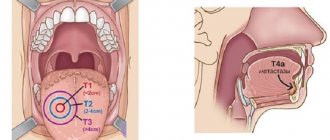
Esophageal carcinoma
In very serious cases, untreated gastroesophageal reflux disease (and subsequent Barrett's esophagus) can lead to esophageal cancer. The main risk factors are alcohol consumption, smoking, poor nutrition, and chronic esophageal diseases with reflux.
Symptoms include weight loss, trouble swallowing, or gastrointestinal bleeding. This is something that happens over decades of untreated reflux (30-40 years), so those who are 30 and otherwise healthy have no reason to suspect cancer. But if you're over 50 and have had heartburn for years and suddenly lose weight, for example, this is definitely what your doctor will suspect first.
Xerostomia in elderly patients: causes, clinical picture, treatment methods
Saliva in its structure is a complex liquid that plays an important role in maintaining an adequate level of dental and general somatic health. It consists mainly of water, and, to a lesser extent, of a variety of inorganic and organic substances such as enzymes, hormones, antibodies, antimicrobial components and growth factors. The specific function of saliva is to ensure the free movement of oral tissues relative to each other, as well as to integrate their combined action during digestion, mechanical chewing, swallowing and speaking. In addition, the proteins that make up saliva are a kind of lubricants for the oral cavity, thus protecting it from various damage of a chemical or physical nature. In turn, enzymes, immunoglobulins A and histamine, also found in saliva, provide local antimicrobial immunity.
Insufficient salivary flow, or general problems with saliva production, which is common among older patients, primarily manifests as a feeling of dry mouth, and is medically referred to as xerostomia. Dysfunction of the salivary glands in elderly patients is most often caused by the influence of systemic diseases, the action of specific medications, and the effect of radiotherapy in the head and neck area.
The prevalence of xerostomia reported by different researchers varies widely, but in general the percentage among patients ranges from 10% to 46% (9.7%-25.8% among men, and approximately 10.3%-33. 3% among women), and in older people over 65 years of age, symptoms of xerostomia occur in approximately 35% of the population.
The presence of xerostomia increases the risk of dental caries, especially root caries, which, in turn, significantly affects the possibility of periodontal diseases and infectious lesions of the oral cavity such as candidiasis. In addition, saliva plays an important role in the adequate functioning of dentures, and signs of xerostomia in prosthetic and already compromised patients can only further aggravate the risk of carious lesions in preserved dental structures. On the other hand, to minimize unpleasant feelings, patients may consume excessive amounts of sweet or sour foods, which, in turn, further increase the cariogenic potential. Considering the high prevalence of xerostomia among the elderly population, doctors must have an excellent understanding of the features of dental rehabilitation of patients with this pathology, as well as their risk of possible complications and consequences after iatrogenic interventions. In addition, only a thorough understanding of the various aspects of this disease will help clinicians most effectively adapt existing prosthetic protocols to achieve the most predictable successful treatment outcome using additional pharmacological and non-pharmacological agents that positively affect the overall outcome of complex therapy.
Causes of the disease
There are three main etiological factors that provoke the development of hyposalivation in elderly patients: specific medications or combinations thereof, direct diseases of the salivary glands, which can occur against the background of such general somatic pathologies as Sjögren's syndrome, diabetes mellitus, and/or Alzheimer's disease, and finally, radiation or chemotherapy to the head and neck area.
Medicines that cause xerostomia
The main reason for the development of xerostomia is the use of specific medications or a combination of them. The effect of polypharmacy often provokes various side effects, including symptoms of hyposalivation, and subsequently a feeling of complete dry mouth. Drugs that cause xerostomia can be found in 42 categories and 56 subcategories of pharmacological categorization, and the most common among these are anticholinergics and sympathomimetics.
Dry mouth can also be caused by tricyclic antidepressants, sedatives, tranquilizers, antihistamines, cytostatics, antiparkinsonian and antiepileptic medications. These agents either inhibit the action of neurotransmitters during their binding to salivary gland membrane receptors or provoke changes in the ion pathway in acinar cells, which can subsequently affect the function of the salivary glands and lead to a hyposalivation effect. The occurrence of xerostomia during chemotherapy is usually temporary: for example, dry mouth may occur as a result of the administration of radioactive iodine used to treat thyroid cancer, but these symptoms normalize over time.
In addition to the above medications, elderly patients often take medications to treat allergies, digestive disorders, or motion sickness. They can also cause dry mouth, which is most likely due not to direct damage to the salivary glands, but to a decrease in salivary flow, and this is mainly due to polypharmacy and the influence of concomitant diseases.
Diseases of the salivary glands
One of the most common somatic diseases that provokes the development of xerostomia is Sjögren's syndrome, an autoimmune idiopathic pathology that affects many tissues and organs. The primary form of the disease is characterized by xerostomia and xerophthalmia (dry eyes), and the secondary form is accompanied by other somatic diseases such as connective tissue lesions, for example, rheumatoid arthritis. Dry mouth is also a common complaint in patients with uncontrolled diabetes, in whom it most often develops due to polyuria and autonomic dehydration. Other diseases that also manifest signs of xerostomia include hepatitis C, lesions of the thyroid gland and adrenal glands. Often, older people with dry mouth also have symptoms of psychogenic conditions, such as depression, stress, or constant anxiety.
Radiation therapy
Complex anticancer treatment often involves radiation therapy, and if it affects the head and neck area, it can easily cause dysfunction of the salivary glands, hyposalivation and xerostomia. Data regarding the prevalence of xerostomia due to radiation therapy vary widely, ranging from 73.5% to 93%. The mechanism of development of pathology under the influence of radiation exposure still remains not very clear, however, most likely the acute form of xerostomia can be caused precisely by the strong inflammatory effect of the X-ray beam, which subsequently provokes fibrosis of the structure of the salivary glands and lysis of acinar cells. Standard radiation used to treat head and neck tumors consists of fractional loads of 10 Gray (Gy) received by the patient every week for one and a half to two months, reaching a total load of 60 Gy units. Although the extent of salivary gland damage depends on the volume of radiation exposure, the duration of radiation, and the area of the face affected, fibrosis and acinar cell lysis have been shown to occur in patients receiving cumulative therapeutic doses greater than 60 Gray. The quality of life in patients after radiotherapy largely depends on the manifestation of xerostomia and the complications associated with it. Research by Kakoei and colleagues showed that for every milliliter of saliva lost, the quality of life index decreases by 2.25%, and although dry mouth in some clinical cases may be temporary, in most patients it is an irreversible process, provoking the emergence of new related problems and complications. Modification of radiation therapy methods and approaches can help minimize the radiation dose to patients, which, in turn, will significantly improve their quality of life during the subsequent rehabilitation period.
Dental complications of xerostomia
The dental status of patients with xerostomia is characterized by many related complications resulting from dysfunction of the salivary glands. Due to a deficiency of saliva, Sjogren's syndrome may begin to develop, the intensity of caries increases, and damage to periodontal tissues progresses. Patients with xerostomia also often experience taste disturbances, which may cause patients to change their normal daily diet and overall eating habits, further contributing to poor oral hygiene. Due to a deficiency of saliva in the oral cavity, ulcers and other traumatic lesions can also often develop, caused by the direct impact of dentures in conditions of complete dryness of the soft tissues.
Also, with xerostomia, new areas of carious lesions appear and existing areas recur, while older patients are most vulnerable to such complications, since more of their own teeth have already been subjected to dental treatment, and areas of gum recession are often observed in the cervical area of these. Recessions especially often occur on the buccal surface of previously restored anterior teeth (photo 1).
Photo 1. View of the oral cavity of a patient with acute carious lesions of the vestibular and cervical surfaces of the teeth, caused by long-term use of anticholinergic drugs.
Without proper salivation and in conditions of disturbed pH levels of the oral cavity, its space is quickly colonized by cariogenic microorganisms, which are the main pathological factor in the development of lesions of hard dental tissues. As for the connection between xerostomia and periodontal diseases, the literature data in this regard are very contradictory. Some researchers have found that the periodontal status of patients with Sjögren's syndrome is similar to that of control patients, while others, on the contrary, claim that the condition of periodontal tissues is worse in patients with xerostomia. The latter argue for an increased risk of periodontal damage due to increased plaque formation due to a deficiency of saliva. In addition, a lack of saliva significantly increases the risk of fungal infections in the oral cavity, especially candidiasis, not to mention the fact that most patients with xerostomia exhibit signs of angular cheilitis and atrophy of the tongue papillae. Being strongly associated with changes in the microflora of the oral cavity, such conditions are caused primarily by Candida fungi, which are present in the oral cavity, on the skin and in the intestines. Interaction with salivary proteins partially helps the body control the colonization of Candida fungi in the oral cavity. The microflora of the oral cavity can change, which leads to a progressive increase in the number of not only opportunistic, but also pathological bacterial agents (photo 2).
Photo 2. Pseudomembranous candidal stomatitis in a patient with xerostomia.
Treatment
The first step in the successful treatment of xerostomia is making an appropriate diagnosis. For example, older patients may have multiple comorbidities and take multiple medications, which in turn may influence the development of xerostomia. Thus, analysis of the patient’s medical history and pharmacological record is a mandatory step to establish the etiology of xerostomia. In addition, in parallel with the diagnosis of xerostomia, the doctor must identify all other lesions in the oral cavity, the treatment of which should be carried out as necessary without interruption from the main therapeutic rehabilitation protocol. Patients with xerostomia are advised to drink as much water as possible and limit their intake of sugary foods that cause caries. After making a diagnosis, the doctor must consider all possible therapeutic options and begin local or systemic stimulation of the salivary glands.
Local stimulation of the salivary glands
Local stimulation of the salivary glands involves the administration of specific saliva substitutes that help reduce the symptom of dry mouth. Saliva stimulants used in North America are typically carboxymethylcellulose-based and generally do not provide long-term results. For example, chewing sugar-free gum is an effective local stimulant because the chewing motion itself increases salivary flow. In addition, you can also use vitamin C, which, according to Bjornstrom's research, provides higher effectiveness than mechanical salivary stimulants. Please note that some researchers claim that ascorbic acid has an adverse effect on tooth enamel, so taking vitamin C should be carefully discussed with your doctor. Adhesive discs, for example, Oramoist, DenTek, can be used as a substance to lubricate and moisturize the tissues of the oral cavity; OraCoat XyliMelts, OraHealth Corporation, or various water-soluble KY Jelly lubricants, Reckitt Benckiser; Taro-Gel, Taro Pharmaceuticals Inc.; Biotene products, GlaxoSmithKline, which can be applied with a brush or directly with your finger. And although these approaches provide different effectiveness in different categories of patients, their main drawback remains their minimal effect precisely at night, when the symptoms of xerostomia are most aggressive.
Systemic stimulation of the salivary glands
Stimulation of salivation can be achieved through the action of specific pharmacological drugs called salivary agents. These medications actually increase salivary secretion and have been shown to minimize the symptoms of xerostomia in dental patients. These include: pilocarpine, cevimeline, bethanechol chloride and anethole trithione. Pilocarpine is a muscarinic antagonist that stimulates cholinergic receptors on the surface of acinar cells. The conducted studies prove the positive effect of pilocarpine in cases of xerostomia that appeared after radiotherapy. In such situations, pilocarpine is taken orally throughout the entire radiation cycle at a dose of 3-5 mg three times a day. Possible side effects: sweating, nausea, dizziness and increased pulmonary secretion. Since this drug can lead to dysfunction of the gastrointestinal tract, as well as the urinary, cardiovascular and pulmonary systems, it should be prescribed with particular caution to persons with inherent bronchial asthma, chronic pulmonary or cardiovascular diseases. Cevimeline is a more potent agonist especially for the M1 and M3 subtypes of muscarinic receptors. Since M2 and M4 receptors are found in cardiac and pulmonary tissues, the use of cevimeline can not only minimize the symptoms of xerostomia, but does not impair the function of the pulmonary and cardiac systems, which was characteristic of pilocarpine. In turn, cevimeline is contraindicated in patients with bronchial asthma and narrow-angle glaucoma. In a double-blind, placebo-controlled study of 200 patients with symptoms of Sjögren's syndrome, Fox demonstrated that cevimeline had a positive effect on salivary flow and improved symptoms of xerostomia. The recommended dose for cevimeline is 30 mg, taken three times a day. Although most of the studies conducted have found that cevimeline is well tolerated by patients, but possible side effects of this drug may include nausea, vomiting, diarrhea, runny nose and increased sweating. Bethanechol chloride has been widely used for the treatment of dry mouth for quite some time, and due to its cholinergic effects, this drug is often prescribed for the treatment of urinary retention and neurogenic atony. Bethanechol promotes salivation through stimulation of the parasympathetic nervous system, which causes the release of acetylcholine at the nerve endings, and, accordingly, provokes the production of saliva.
In a recent double-blind, randomized, prospective study, Jaguar, examining the prophylactic use of bethanochol to prevent salivary gland dysfunction during radiation therapy in 97 patients, demonstrated the positive effect of this drug by reducing the degree of damage to the salivary glands by X-ray irradiation. Bethanechol chloride is administered in doses of 10 mg to 50 mg three to four times daily. Previously reported side effects of the drug include gastrointestinal disorders, sweating and miosis. Anethole trithione promotes an increase in receptor sites on the surface of acinar cells. A study conducted by Epstein showed that patients taking anethole trithione had an improvement in salivary flow, and in addition, concomitant use of anethole and pilocarpine was shown to have a synergistic effect that improves overall treatment outcome. The recommended dose of the drug is 25 mg when taken three times a day. Possible side effects include gastrointestinal disorders, flatulence, bloating and pain.
Conclusion
Salivation levels decrease significantly with age, which in turn can lead to the development of xerostomia. Such dysfunction in geriatric patients is largely due to the influence of various systemic diseases, the effects of medications, and side effects of radiation therapy to the head and neck area. This article discusses the main reasons for the development of this pathology, as well as its consequences, and also presents possible treatment options for xerostomia, as an extremely important dental disease. The clinician’s task is to diagnose xerostomia in a timely manner and select the most adapted algorithm for its treatment, depending on the etiology and general somatic condition of the patient.
Author: Aviv Ouanounou, BSc, MSc, DDS