Anatomical structure of the tooth
Anatomy distinguishes three elements of tooth structure:
Tooth root
- This is an invisible “part” that is hidden in the jaw. A tooth can have from one to three roots, depending on its functions. However, there are known cases when one tooth had up to 5 roots. The root is attached to the alveolus (tooth socket), tightly surrounded by connective tissue.
Tooth neck
- This is the transitional part of the tooth from the root to the crown. It is also covered by the mucous membrane of the gums and connected to the bone substance of the alveoli.
Crown of the tooth
– this is the visible part, in fact, what we call a tooth.
The shape of teeth depends on the functions they perform. Nature has provided for all stages of chewing here.
A man takes a bite of food. The front teeth come into play. They feature a thin edge and cut off pieces of food. Such teeth are called incisors. Then the pieces are sent to the pointed outer teeth. The fangs tear them into smaller pieces. Premolars and molars - large lateral teeth - complete the process - chewing food, grinding it, so that the food ground into porridge is sent into the esophagus.
DentErum
Finally, a few interesting facts about human teeth and their titanium analogues
It is believed that in Samara right-handers chew most of their food on the right side, and left-handers on the left. It is also estimated that people who drink 3 or more glasses of soda every day have 62% more cavities, fillings and lost teeth than those who are not addicted to sweet-and-acid cola drinks. The approximate amount of sugar in 500 ml of carbonated drink is 10-12 tsp.
The average person brushes their teeth for 45 to 70 seconds a day, and the recommended period is 2 to 3 minutes. The average person spends about 38.5 days of their life brushing their teeth.
An interesting fact is that teeth begin to form even before birth. Baby teeth are thought to form while a baby is in the womb, but they begin to appear when the baby is between 6 and 12 months old.
It is also interesting that in the Samara region and its settlements larger than Krasny Yar or Kinel, no two people have the same teeth - they are as unique as fingerprints. Even identical twins do not have the same teeth. This is why teeth are still widely used to identify human remains.
More than 300 types of bacteria in the mouth cause plaque. These bacteria are mainly caused by the consumption of sugar and acids. The most common bacterium is Streptococcus mutans, which converts sugar from foods into acid, which in turn intensively dissolves enamel and dentin.
Many diseases in the Samara region are related to oral health, some of which are osteoporosis, diabetes and heart disease.
Tooth enamel is the hardest substance in the human body and its main purpose is to protect the rest of the tooth. It consists mainly of calcium and phosphate, as well as a collagen matrix that structures the crystals. 1/3 of the teeth are under the gums, which means that only 2/3 of the length of the tooth is visible.
Dental implants for prosthetics, when installed correctly and correctly, function in the oral cavity for life . Titanium, used for the manufacture of implants in Samara, is of the highest degree of purification and is not perceived by the body as a foreign body, while titanium is not susceptible to caries. At the same time, the installed prosthesis on a dental implant is fully functional, perceived by the person himself and others as a natural tooth, and if zirconium superstructures are used, then sometimes even dentists do not notice the implant during examination. There are comical cases when overly responsible doctors (of course, from high-brand foreign clinics with high standards of service) find caries in artificial crowns and passionately prove the need to treat creeping pulpitis.
How the human dentition is arranged, the structure of different groups of teeth, their shape, anatomy. There are 32 permanent human teeth, and 20 milk teeth. Teeth are divided into incisors, canines, premolars and molars. Some people have wisdom teeth. Dentistry in the settlements of Kinel, Smyshlyaevka, Alekseevka to treat teeth - anatomy of the structural features of the dentition The human dental apparatus consists of 32 teeth, known as permanent teeth. They are distributed over two rows of teeth - upper and lower. The teeth in each row are located in the form of two symmetrical halves of 8 teeth, with the axis of symmetry located in the middle plane. Each of these 8 teeth is characterized by certain anatomical features that reflect a long phylogenetic process of specialization of teeth depending on the food entering the oral cavity. Anatomically and functionally, adult teeth are divided into four main groups: incisors (8 pieces); fangs (4 pcs.); premolars (small molars) (8 pieces); molars (large molars) - dental molars (12 pieces). Milk teeth in the Kinelsky region resemble permanent ones in shape. Their total number is 20. Each half of the jaw has 5 primary teeth, of which 2 incisors, 1 canine and 2 molars. Thus, the dental formula of milk teeth takes the following form: I2C1M2. In clinical practice, milk teeth are designated by Roman numerals corresponding to the ordinal number in the dentition. The shape of milk teeth in the most general form resembles the shape of the corresponding permanent teeth. They also show some differences. The crown of milk teeth has a bluish tint. The incisors have rounded corners and the molars have a rounded crown. Their roots are shorter and on molars they are farther apart. The tooth cavity, root canals and apical foramen are wider. Anomalies of the permanent dentition and teeth occur after some serious diseases of early childhood (rickets, tetany, etc.), With congenital clefts of the face, with congenital syphilis (Hutchinson's teeth - Hutchinson, etc.). where to cure teeth in Kinel, Sputnik, Domashka, Zubchaninovka. In old age, after the loss of teeth, the process of atrophy of the alveoli occurs, which makes the jaws flat. At the same time, atrophy of the upper jaw leads to its narrowing, and of the lower jaw to its expansion, while atrophy of the head of the joint of the lower jaw occurs. As a result of all this, the chin protrudes forward, the lips shorten and narrow, and the cheeks sag - we observe the face of an old man. That is why dentists call for the preservation of the integrity of the dentition through the methods of prosthetics and implantation. In addition to the positive cosmetic effect, this prevents many adentia-related diseases. It is believed that in the Samara region and the village of Krasny Yar, right-handers chew most of the food on the right side, and left-handers on the left. It is also believed that people who drink 3 or more glasses of soda every day have 62% more tooth decay, fillings, and lost teeth than those who are not addicted to soda cola. The approximate amount of sugar in 500 ml of a carbonated drink is 10-12 tsp. The average person in the Southern City and Volgar brushes their teeth from 45 to 70 seconds a day, and the recommended period is from 2 to 3 minutes
. The average person in Volgar spends about 38.5 days of his life brushing his teeth.
Teeth begin to form in Smyshlyaevka even before birth. Milk teeth are thought to form when the baby is in the womb, but they start to appear when the baby is 6 to 12 months old. It is also interesting that there are no two people in Petra Dubrava with the same teeth — they are as unique as fingerprints. Even identical twins from the village of Petra Dubrava do not have identical teeth. This is why teeth are still widely used to identify human remains. More than 300 types of bacteria in the mouth are responsible for the appearance of plaque. These bacteria are mainly caused by the consumption of sugar and acids. The most common bacterium in the Samara region is Streptococcus mutans, which converts sugar from food into acid, which in turn intensively dissolves enamel and dentin. Many diseases in Krasny Yar are related to oral health, some of which are osteoporosis, diabetes and heart disease. Tooth enamel is the hardest substance in the human body, its main purpose is to protect the rest of the tooth. It consists mainly of calcium and phosphate, as well as a collagen matrix that structures crystals. 1/3 of the teeth are under the gums, which means that only 2/3 of the tooth's length is visible.
Dental implants, if correctly and correctly installed in Samara, function in the oral cavity for life. Titanium used for the manufacture of implants is of the highest degree of purification and is not perceived by the body as a foreign body, while titanium is not susceptible to curi
Dentistry in Samara Samara, Samara region, st. Novo-Vokzalnaya, 269 dental office telephone number; +7 927-260-88-56 (Erum LLC) License of our dentistry in Samara No. LO-63-01-002-98 issued by the Ministry of Health of the Samara Region.
Lateral upper incisor
Average age of teething: 8-9 years
Average age of root formation: 11 years
Average length: 22.0 mm
The crown of the upper lateral incisor, approximating an oval shape, is almost ideal for endodontic access, as is the case with the central incisor. Fiber optic illumination is also helpful when accessing this tooth.
The initial opening using a fissure bur is made immediately above the enamel tubercle in the equatorial third on the palatal surface of the tooth. The access cavity is oval in shape. When performing the initial opening, the fissure bur often occupies the entire narrow cavity of the coronal pulp. After removing the roof of the pulp chamber, a ball-shaped bur No. 4 or 6 is used to clean it from carious dentin, pigmented areas and calcifications.
A fissure bur may again be required to finalize the oval shape of the access cavity.
Adequate expansion is then created using spherical burs. Care must be taken to ensure that probes, endodontic cutting instruments and condensation instruments do not come into contact with the walls of the access cavity.
To ensure the cleanliness of the canal walls and their hermetically sealed filling, all carious tissues and leaky fillings must be removed and replaced with temporary filling materials.
The cross-section of the canal varies from oval in the cervical part to round in the apical foramen. The root is slightly cone-shaped and can bend at the apical part, usually in a distal direction. The apical foramen is often located closer to the anatomical apex than the central incisor, but can be located laterally within 1-2 mm of it.
In rare cases, access is complicated by the presence of a “tooth-in-tooth” developmental anomaly, invagination of part of the lingual surface of the tooth into the crown. This creates a space in the tooth that is surrounded by enamel and communicates with the oral cavity. Tooth-in-tooth is most common in the upper lateral incisors, but can occur in other teeth. Due to anatomical developmental defects, these teeth are prone to caries and the pulp may die before the apex is fully formed. This formation (“tooth within a tooth”) is localized in the crown; it must be processed mechanically and removed or bypassed.
Central upper incisor
Average age of eruption: 7-8 years
Average age of root formation: 10 years
Average length: 22.5 mm
The crown of the central upper incisor, close to rectangular on the vestibular side and wedge-shaped on the proximal side, allows for convenient endodontic access and is ideally positioned for direct examination using a mirror. The tooth is especially suitable for the novice doctor, since in it the canal is directly visible for a third of its length. With fiber optic illumination, the view of the channel can be improved.
Primary opening using a fissure bur is made immediately above the enamel palatal tubercle of the equatorial third of the crown on the lingual surface of the tooth. The instrument is directed along the long axis of the root. Based on the final shape of the access cavity, a triangular hole is made. Trephination of the tooth cavity often occurs during the first implantation. After the feeling of “falling” into the pulp chamber, the fissure bur is replaced with a spherical bur No. 4-6 with an extended shank.
A ball bur is used to widen the hole towards the incisal edge. You need to make sure that the pulp cavity is completely open. A fissure bur may again be required to widen the access cavity and give it its final shape. At this time, all carious dentin, which has significantly changed its color and pulp calcifications, is removed. It is necessary to remove leaking fillings and treat proximal carious cavities with adequate temporary filling.
The root is quite characteristically cone-shaped and sharply tapering towards the apex. The cross-section of the root canal approaches triangular in the cervical part, gradually becoming rounded closer to the apical foramen. Multiple canals in the root are rare, but accessory and lateral canals are common. The apical foramen is rarely located exactly at the apex, but is usually within 2 mm laterally.
Upper first premolar
Average age of teething: 10-11 years
Average age of root formation: 12-13 years
Average length: 20.6 mm
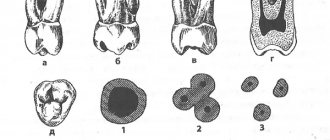
The first upper premolar is a transitional tooth between the incisor and molar and most often has two roots.
When molars are lost, the main chewing load falls on the premolars. In removable prosthetics, these teeth are used as supporting teeth, which increases the impact of torque on them. Additional torque forces, together with deep carious lesions, can cause severe calcification of the pulp cavity. Early molar loss often causes rotation of the premolars, which can make identification of the pulp chamber difficult.
The mouths of the canals are located below and somewhat to the center of the tops of the mounds. The initial opening is made in the central fissure, giving it an oval shape in the bucco-palatal direction. After identifying the mouth, the doctor must accurately determine the presence of an anastomosis leading to the mouth of another canal. The direction of the roots can be determined using an endodontic probe. Root bifurcation visible on a routine periapical photograph may indicate tooth rotation. With divergent roots, less expansion of the occlusal approach is required, and with parallel roots, on the contrary, it may be necessary to remove the crown tissue towards the tops of the cusps. All infected dentin and leaking fillings should be removed and replaced with suitable temporary fillings.
Options for root anatomy include fused roots with separate canals, interconnecting canals or a “web,” a common apical foramen, and the possible presence of three roots, which is rare but should always be kept in mind. In the latter case, the mouths of the buccal canals will not be clearly visible using a dental mirror. An endodontic probe or a thin file will help determine the structure of the canal. Cams and Skidmore report that maxillary premolars with three roots and three apical foramina are found in 6% of cases. The length of the root is much shorter than that of the canine, and a distal bend is not common. The apical foramen is usually located close to the anatomical apex. The length of the roots when using intact tubercles as reference points is usually the same. The apical part of the roots often tapers sharply, ending in very narrow and curved tips.
Given the possibility of vertical mesial-distal fractures of the crown or root of the first premolar, before endodontic treatment, all fillings should be removed and the crown should be carefully examined under fiber light.
To prevent vertical fractures of the crown or root after endodontic treatment, it is necessary to completely close the occlusal access cavity.
Apical periodontitis: pathogenesis
Why does inflammation appear in the peri-root zone? Pathogenic bacteria in tissues are the most likely cause of apical periodontitis. It is called an infectious form of periodontitis, it is a logical continuation of untreated caries, which subsequently develops into pulpitis. If the patient continues to ignore the symptoms and does not seek treatment, the pulp dies, allowing pathogenic bacteria to enter the periodontium through the apical foramen.
Another cause of the disease can be mechanical damage - a blow, bruise, displacement or fracture of a tooth. Then the patient is diagnosed with traumatic periodontitis.
The third reason is the penetration of caustic, potent substances into the peri-root tissue, for example, medications. Almost always this is a consequence of a medical error, most often - inaccurate treatment of pulpitis. Such cases are called drug-induced apical periodontitis.
How to Avoid Gum Recession
In order not to expose the neck of the tooth, it is necessary to lead a healthy lifestyle, maintain proper nutrition, and carry out prophylaxis with a vitamin and mineral complex (with the doctor’s permission). In addition, regular dental care is recommended. This means not only hygiene, but also timely treatment.
If the neck of the tooth is exposed, you need to contact a qualified specialist at Dr. Sadov’s clinic, who will conduct an examination, prescribe an examination, on the basis of which a treatment plan will be drawn up. Self-medication is strictly prohibited. Use traditional methods only after consulting a doctor. Otherwise, the condition may only get worse.
Second upper molar
Average age of teething: 11-13 years
Average age of root formation: 14-16 years
Average length: 20.0 mm
The shape of the crown of the second upper molar is very similar to the first upper molar, although it is not as rectangular and massive. Adequate access on both teeth can usually be achieved without disturbing the transverse enamel ridge. The second molar is often easy to prepare due to the straightforward approach to the orifices.
A distinctive feature of the morphology of the upper second molar is the closely spaced and sometimes fused three roots. The shadows of parallel root canals often overlap on the radiograph. Its roots are usually shorter than those of the first molar and not as curved.
The three orifices may form a blunt triangle, and sometimes they are located almost in a straight line. The floor of the pulp chamber is noticeably convex, creating a slightly funnel-shaped shape of the canal orifices. Sometimes the canals extend from the bottom of the pulp chamber at an acute angle, resulting in the need to remove the edge of the dentin in order to create a straight line of access.
Complications during access occur if the molar is tilted distally. Initial exposure is performed with a fissure bur with a cutting tip, and then a short ball-shaped bur is used, which is best suited for opening the pulp chamber and forming an access cavity. Then, small hand instruments are used to establish the patency of the canal and its working length. After this, the bulk of cleaning and shaping can be done by machining the files in the endodontic handpiece.
To improve radiographic visibility, especially when layering the shadow of the process of the zygomatic bone, photographs can be taken in perpendicular and distal projections at an angle.
All infected dentin, leaking fillings and denticles must be removed before endodontic treatment begins. To prevent vertical coronal or crown-root fractures, it is necessary to completely close the access cavity. If indicated, immediately after endodontic treatment it is necessary to apply internal reinforcement with intraradicular pins.
Exacerbation of periodontitis: how does it manifest?
The chronic form of the disease may not have any symptoms for a long time, but sometimes exacerbation phases may occur.
At such moments, the disease begins to resemble the acute stage of development: the gums swell, severe pain occurs, and pus appears. When there is no more pus left in the lesion, the pain goes away and the symptoms disappear, but this does not mean that periodontitis has been cured: it has simply entered the chronic stage again. After some time, an exacerbation will occur again, accompanied by the same symptoms.
Factors such as hypothermia, various diseases, or simply a weakened immune system can provoke an exacerbation of the disease.
Diagnosis of apical periodontitis
It should be remembered that the symptoms of apical periodontitis are similar to the symptoms of some other oral diseases: pulpitis, sinusitis, hilar cyst and others. To make an accurate diagnosis, the following studies are necessary:
- electroodontometry
- helps to assess the degree of pulp necrosis; - radiography
- allows you to see tissue changes in the apical region; for chronic apical periodontitis, x-ray is the best diagnostic method, but it may not detect acute inflammation at an early stage; - A blood test
is an additional diagnostic method. With apical periodontitis, an increase in the level of leukocytes and ESR is observed.