Inflammatory processes that form around the root are very dangerous, because they not only destroy the cement of the root and the adjacent bone tissue of the jaw, but also affect the gums. If a dentist discovers a cyst, then soon a trip to the surgeon will be necessary, but this does not mean that the patient will lose a tooth. At the Implantmaster clinic, cyst removal is performed without tooth extraction. Our specialists use the latest surgical techniques and equipment.
Removal of a dental cyst is a serious operation in dental surgery. Two decades ago, the presence of a purulent formation on the root led to the removal of a possibly healthy tooth. Modern treatment options for cysts are more varied. There are many therapeutic (conservative) and surgical methods to combat tumors. If doctors have the necessary knowledge and professional skills, patients can count on receiving quality treatment.
In the innovative dental clinic "Implantmaster" in Moscow, cyst removal is carried out by specialists of the highest category, who regularly improve their skills in the best clinics in Europe. We are able to solve complex problems in the fastest possible time and satisfy the needs of even the most demanding patients, setting loyal prices for the services provided. Our doctors are constantly improving their skills, mastering new techniques for removing cysts. The latest materials are used, modern equipment is used for diagnosis and treatment.
Next we will talk about the very concept of “cyst” and methods of its treatment. You will also learn about the main stages of removing a dental cyst, and will be able to get acquainted with the indications for the surgical operation.
What is a dental cyst and how to remove it?
Radical dental cyst is a complex chronic disease. It has its own shell and is filled with purulent contents. The disease progresses on the roots and under the gum. A cyst appears when early infectious inflammation, which is based on pathogenic microflora, is not treated.
Removal of a dental cyst is performed surgically . The tumor can grow, affecting the gums and cheeks from the inside of the mouth. In some cases, sepsis may develop.
All this makes it difficult for the patient to function normally. To cure the disease, conservative methods are used:
- at the beginning of the procedure, the doctor informs the patient about the possible consequences (it is worth making this the first point);
- the doctor performs an opening of the dental cavity;
- cleansing the cavity from affected tissues;
- treatment with solutions of antibiotics and antiseptics;
- Then, within half an hour, the tooth cyst is removed without removing the tooth .
The patient will have a chance for recovery and further normal life. The main feature of this disease is its asymptomatic course. The patient may remain unaware for a long time. The consequences of this disease can lead to another complex process - sinusitis (if the cyst is located near the sinuses). It is imperative to monitor the cleanliness of the oral cavity and the condition of the gums, and also come to the doctor for sanitation on time.
The need for the procedure
Cystectomy in dentistry is performed to:
- Remove benign encapsulated tumor.
- Restore the structure of a unit of the dentition, which is subject to blackening, destruction and loss.
- Eliminate pain and bleeding that accompany the inflammatory process in the gums.
- Remove purulent neoplasm. This is the previous step before implantation or prosthetics. Provided that the cyst has reached a large size, and there is no possibility of saving the tooth root.
- Eliminate a progressive cyst.
- Relieve the inflammatory process, the symptoms of which are pain, bleeding, and accumulation of pus.
Patients should be aware that if surgery is not performed in a timely manner, the inflammatory process will intensify, resulting in the destruction of dental tissue. If the cyst is not removed, it can transform into a malignant tumor.
Causes of dental cysts
Ten percent of patients have indications for removal of a dental cyst. Most do not suspect anything, because the disease proceeds secretly for a long time and does not manifest itself in any way. Often, cyst formation is a hereditary disease, and sometimes it indicates poor oral hygiene. But more often the reasons are untreated diseases or the use of low-quality products and drugs, leading to the need to remove the dental cyst. If you identify this disease in time and immediately consult a doctor, it will not be difficult to cope. But if you leave a formation with pus and mucus for several months, it can grow up to 2-3 cm. In this case, proper surgical removal of the dental cyst should be entrusted to a qualified specialist.
Implantmaster employs highly qualified specialists; they have the necessary skills for comfortable and high-quality treatment. Also, to correctly diagnose the disease and determine the exact size of the cyst, the clinic has a CT scanner (the images are more accurate and the radiation is even less), it is possible to take a panoramic image of all teeth, as well as targeted radiography of a specific tooth. The diagnosis becomes more accurate.
There are several causes of cysts:
- A complicated form of caries is severe destruction of the enamel, through which microbes penetrate inside and form purulent foci.
- Untreated pulpitis, when part of the nerve is outside, is a good flora for the growth of bacteria.
- The complication of periodontitis, with inflammation of the connective tissue, is the most difficult to detect.
- Removal of a dental cyst is often necessary for children when replacing milk teeth with permanent ones; microbes can penetrate into the sockets.
- The injured mucous membrane of the palate, cheeks, tongue, and gums can serve as an excellent route for the penetration of microorganisms.
- Past disease of the ENT organs. Colds, chronic tonsillitis, pharyngitis, sinusitis can cause a tumor and the need to remove a dental cyst, otherwise dangerous complications cannot be avoided.
When not to have surgery
There are some factors, the presence of which is a contraindication to dental cystectomy; the price is about 7,000 rubles. These include:
- If the purulent tumor has reached a large size, under the influence of which several elements of the dentition have fallen, as a result their structure has been disrupted, suppuration and the inflammatory process have begun.
- If a patient is diagnosed with an infectious disease or inflammation, which has caused the destruction of the structure of the teeth, their loosening, as a result, periodontitis or periodontal disease begins to develop.
- For oncological or endocrine disease, the occurrence of which is associated with an inflammatory process in the gum or tooth root. These diseases include leukemia, sarcoma, and diabetes.
- When the tooth crown is destroyed, blackened, resulting in suppuration. Causes include infectious disease and bad habits in humans.
When is it necessary to remove a dental cyst?
Is surgical removal of a cyst on a tooth necessary? In some cases, such a radical method cannot be avoided. If the affected tissue is not eliminated, the bubble with purulent contents will increase in size and create pressure on the gum. The outcome may be tumor formation.
Indications for removal:
- capsule diameter is more than 1 cm;
- the presence of a pin in the root canal, which prevents refilling;
- the canal is not completely sealed, there is no material near the very top;
- Conservative treatment is not effective.
Execution technique
Cystectomy is performed under general anesthesia, which not only anesthetizes, but also bleeds the surgical field. Next, the following activities are performed:
- bone exposure;
- gaining access to the cyst;
- removal of the formation (in case of union with the root, its resection is performed);
- filling;
- antibacterial treatment of the bone cavity;
- suturing.
To prevent the appearance of a hematoma, a pressure bandage is applied to the operated area, which is removed after 5-7 days.
Subsequently, the patient is prescribed treatment with anti-inflammatory, antiallergic and painkillers.
Methods for removing dental cysts
Correct treatment of a dental cyst without removal depends on the causes and clinical course. The clinical picture becomes clear after examination in a chair, a targeted photograph, a panoramic photograph of all teeth, . These examination and diagnostic methods for the necessary removal of a dental cyst are available at Implantmaster in Moscow. Examinations are performed before surgery to determine the specific location of the inflammation. If possible, conservative therapy is used to prevent further increase in inflammation. It consists of using a rubber dam to isolate the working field and provide comfort during treatment. Next, the pulp chamber is opened, cleaned, treated with an antiseptic solution and the canals are sealed. Therapy involves taking antimicrobial drugs, vitamins and other medications. If conservative tactics are not effective, then various surgical techniques are used to remove the tooth cyst without removing the causative tooth.
Cystotomy
Used for large cysts. The doctor removes parts of the formation that are not in contact with the vessels. Afterwards, an obturator is installed into the resulting cavity - a device that prevents tissue fusion. After some time, the remaining portion of the cyst joins the epithelium of the oral cavity, changes its structure and becomes safe for the body.
Hemisection
During the operation, the root to which the formation is attached and the adjacent coronal part are removed. The resulting space is restored using an orthopedic structure. The above method is quite traumatic, so it is considered outdated.
.
Cystectomies
The Implantmaster clinic answers the question: is it possible to cure a dental cyst without removing the tooth itself? – positive. Our specialists use the most modern technique - cystectomy. The tumor is completely removed without affecting healthy tissue. The operation takes place under local anesthesia in the surgical office and involves the use of a Labomed Magna dental microscope.
At the beginning of the procedure, the specialist determines the location of the patient’s formation based on examination and x-ray images. He “opens” it, cleans out the contents with special tools, puts antiseptic inside and stitches it up. After some time, the cavity remaining after the operation heals on its own, without requiring additional replanting of bone blocks. Cystectomy surgery takes 15-40 minutes, depending on the size of the cyst and bone structure. After an hour, the patient can go home.
Contraindications
The patient will be denied manipulation if certain conditions are present:
- the root is located in the cyst by more than a third;
- inflammatory process on the mucous membranes, which threatens infection of the soft tissues during the incision;
- destruction of the crown part of the tooth;
- malignant tumors;
- small bone volume, which increases the risk of bone damage.
Also, the patient will be denied surgery if there are standard contraindications for surgery: diabetes, infectious diseases, vascular diseases, pregnancy, etc.
Get a consultation
We will answer all your questions before visiting the clinic!
+7
Online registration
Removal of a dental cyst by resection
Removal of a dental cyst by resection of the root apex is a tooth-saving operation, i.e., making it possible not to part with the tooth. It is carried out by excision of the root and removal of the affected fragments. Then, to avoid the spread of infection to adjacent areas of hard and soft tissue, the canal is sealed. As a result, this is a good way to cure a dental cyst at the initial stage without removing the entire unit. If a fragment of the tooth remains, it will be replaced with prosthetics in the future. Tooth-preserving methods are valued by specialists because they help preserve the integrity of the dentition. Therefore, resection of the root apex is also used in other cases:
- Inflammation of the tooth under the crown. The obvious solution is to remove the prosthesis, remove the abscess, and install a new design. However, these manipulations are more costly and time-consuming than root resection.
- Root canal abscess, often irregularly shaped, due to unscrupulous filling or the use of low-quality materials.
- With osteomyelitis. There is a need to cut out the affected areas of bone tissue at the border with the roots. This helps prevent deep infection.
- When foreign objects are detected in the channels - boron particles, files. This happens when using low-quality equipment. Our clinic uses the latest instruments based on titanium alloy.
However, such an effective operation has contraindications. Removal of a dental cyst by resection is not carried out if: diseased and healthy roots are located critically close; in the presence of extensive chips of the crown; high tooth mobility; in the stage of acute periodontitis. Not recommended for people with diabetes, mental and nervous disorders, chronic heart and vascular diseases, pathologies of the lungs and thyroid gland.
What to do during the recovery period
After surgery, swelling, pain, and inflammation may be observed in the area of the gum where the cyst was removed. If the patient conscientiously follows the doctor’s recommendations, the symptoms will disappear after a short period of time. To avoid negative consequences and re-development of the disease, the doctor recommends following some rules:
- To brush your teeth, you need to purchase a brush that will not cause bleeding or irritation of the gums.
- The diet that must be followed during the recovery period should not include solid, overly hot or cold foods. In addition, avoid consuming foods that are not capable of causing irritation of soft tissue, which, in turn, will cause a re-inflammation process.
- The patient should give up bad habits that can negatively affect the integrity of the teeth and soft tissue after cystectomy. It is not recommended to smoke or drink alcoholic beverages.
- It is necessary not to take medications that can cause an allergic reaction or are included in the list of other contraindications. With such a reaction of the body, the structure of the teeth and soft tissues will be disrupted.
If the patient carefully follows all medical recommendations, the risk of re-formation of the cyst and inflammation will be reduced.
How is surgical removal of a dental cyst performed?
How is the operation to remove a dental cyst performed? It includes the following steps:
- Making a diagnosis using x-rays to determine the size of the capsule and the condition of the roots.
- Conducting local anesthesia.
- Cutting and peeling of the gums.
- Drilling out a bony area in the body of the jaw for better access to the formation.
- High-quality cleaning of the contents of the capsule and removal of its shell to prevent further illness.
- Rinsing the cavity with antiseptics.
- In some cases, if necessary, removal of part of the affected root and retrograde filling of the canals.
- Filling the cyst location with osteoplastic material (artificial bone).
- Suturing the mucous membrane.
- After the procedure, it is mandatory to take a control X-ray to ensure that the operation was carried out properly (all infected tissues were removed).
A tooth is removed if its roots are in a cystic formation or if it is completely destroyed.
More about the procedure
Cysts most often form near the roots of teeth; without treatment, they can grow rapidly and involve surrounding tissues. Drug therapy is effective at the initial stage, when there is an inflammatory process, but there is no formed capsule. When a tumor appears, surgical treatment is recommended.
Cystectomy is a tooth-preserving operation during which the cystic formation and the mobile part of the root around it are removed. The technique allows you to excise the cyst, which eliminates the possibility of a secondary appearance of a formation in this place. It is performed on both the lower and upper jaws.
Laser removal of dental cyst
If the tumor is small, then laser removal may be used. This is a simple and safe way. A laser beam is passed through the root canal, sterilizing it, and the cyst gradually reduces in size.
Positive aspects of using laser:
- not painful and bloodless;
- fast regeneration;
- disinfection of the inflamed area and, as a result, reducing the risk of spreading bacteria.
The disadvantages include the high cost of the procedure, as well as the availability of a laser device not in all clinics.
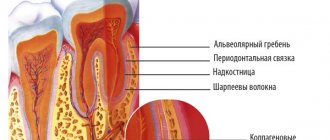
A cyst is a cavity with a shell, which consists of an outer connective tissue layer and an inner layer, lined predominantly with stratified squamous epithelium. The cyst cavity is usually filled with a yellow liquid, opalescent due to the presence of cholesterol crystals in it, sometimes with a cheesy mass of gray-dirty-white color (with a keratocyst). Its growth is due to intracystic pressure, which leads to atrophy of the surrounding bone tissue and proliferation of the epithelium. The etiopathogenesis of odontogenic cysts is different. A cyst, the development of which is based on an inflammatory process in the periapical tissue, is called root (radicular). It can be apical (apical) and lateral, as well as residual (residual) after removal of the “culprit” tooth. A paradental cyst is formed when the eruption of a wisdom tooth is difficult.Other cysts are a malformation of odontogenic epithelium. Among them are the primary cyst (keratocyst), tooth-containing (follicular), eruption cyst and gingival cyst.
Jaw cysts occupy first place among other odontogenic formations. They occur in people of all ages and form on the upper jaw 3 times more often than on the lower jaw. Clinical and radiological manifestations of various odontogenic cysts and methods of their treatment have much in common. However, each type of cyst has characteristic features that allow them to be differentiated from each other.
Root (radicular) cyst. The occurrence of a root cyst is associated with the development of a chronic inflammatory process in the periapical tissue of the tooth. The latter contributes to the formation of granuloma. Inside this granuloma, epithelial remnants (islets of Malasse) of the periodontal ligament, activated by inflammation, proliferate, which first leads to the formation of cystogranuloma and then cysts.
Clinically, a root cyst is usually found in the area of a destroyed or treated tooth, and sometimes in a seemingly healthy one, but previously exposed to trauma, less often in the area of an extracted tooth (residual).
The cyst grows slowly over many months and even years, unnoticed by the patient, without causing any discomfort. It spreads mainly towards the vestibule of the oral cavity, while thinning the cortical plate and leading to bulging of the jaw area.
When a cyst arises from a tooth whose root faces the palate, thinning and even resorption of the palatal plate is observed. A cyst that develops within the boundaries of the maxillary and nasal cavities spreads towards them. Upon examination, a smoothness or bulging of the transitional fold of the arch of the vestibule of the oral cavity of a round shape with fairly clear boundaries is revealed. When localized on the palate, limited swelling is noted. By palpation, the bone tissue over the cyst bends; with sharp thinning, the so-called parchment crunch (Dupuytren's sign) is determined; in the absence of bone, fluctuation. The teeth located within the boundaries of the cyst may be displaced, then their crowns converge, and when the causative tooth is percussed, a dull sound occurs. Electroodontodiagnosis (EDD) of intact teeth located in the cyst zone reveals a decrease in electrical excitability.
Often a cyst is diagnosed when its contents suppurate, when inflammation of the surrounding tissues develops, such as periostitis; Vincent's symptom may be observed - numbness of the lower lip due to involvement of the lower alveolar nerve in the acute inflammatory process. When a cyst forms on the upper jaw, chronic inflammation of the maxillary sinus is possible.
The X-ray picture of a root cyst is characterized by rarefaction of bone tissue of a round shape with clear boundaries. The root of the causative tooth is located in the cavity of the cyst.
The relationship of the roots of adjacent teeth with the cystic cavity may vary. If the roots protrude into the cavity of the cyst, the periodontal fissure is absent on the radiograph due to resorption of the endplate of the sockets of these teeth. If the periodontal fissure is identified, then such teeth are only projected onto the area of the cyst, but in fact their roots are located in one of the walls of the jaw. In some cases, the roots of the teeth are pushed apart by the growing cyst. Root resorption, as a rule, does not occur.
A large cyst of the lower jaw thins the base of the latter and can lead to a pathological fracture. A cyst growing towards the bottom of the nose causes destruction of the bone wall. The cyst located within the boundaries of the maxillary sinus has a different relationship with its bottom. Preservation of an unchanged bone floor is characteristic of a cyst adjacent to the maxillary sinus. Thinning of the bony septum and its dome-shaped displacement are characteristic of a cyst pushing back the sinus.
A cyst penetrating into the sinus is characterized by the absence of a bone wall, with a dome-shaped soft tissue shadow against the background of the maxillary sinus.
Diagnosis of a root cyst based on clinical and radiological picture usually does not cause difficulties. In doubtful cases, puncture of the cyst and cytological examination of the contents are performed.
Microscopically, the shell of the root cyst consists of fibrous tissue, often with inflammatory round cell infiltration, lined with non-keratinizing multilayered epithelium.
Treatment is surgical. Cystectomy, cystotomy, two-stage surgery and plastic cystectomy are performed.
A primary cyst (keratocyst) develops mainly in the lower jaw, is observed relatively rarely, begins unnoticed and does not appear for a long time. Upon examination, a slight painless bulging of the jaw area in the area of one of the large molars is detected. In some patients, the cyst is detected due to the addition of an inflammatory process, sometimes it is found by chance during an X-ray examination for other diseases.
The keratocyst spreads along the length of the jaw and does not lead to significant bone deformation. Therefore, it is determined when it reaches large sizes. The cyst extends to the body, angle and ramus of the jaw.
The X-ray picture is characterized by the presence of extensive bone loss with clear polycyclic contours, while uneven bone resorption creates the impression of multi-chamber. Often the coronoid and condylar processes are involved in the process. The cortical plate becomes thinner and is sometimes absent in some areas. An x-ray usually reveals the periodontal gap in the roots of the teeth, projecting onto the area of the cyst.
A primary odontogenic cyst is diagnosed based on characteristic clinical and radiological manifestations. It should be differentiated from ameloblastoma. With the latter, pronounced swelling of the jaw is observed. The final diagnosis is established after a morphological examination of the biopsy material. An open biopsy is performed with mandatory excision of the bone tissue and cyst shell according to the type of cystotomy. A biopsy is also the first stage of surgical treatment of a cyst.
Macroscopically, the primary odontogenic cyst is a single cavity with bay-shaped impressions into the surrounding bone, covered with a membrane and made of an amorphous mass of off-white color. Microscopically, it is characterized by a thin fibrous capsule lined by keratinizing stratified squamous epithelium.
Treatment is surgical. Since the cyst is capable of recurrence and malignancy, complete removal of its shell is indicated while preserving the bone walls. In other cases, a two-stage surgical method is used.
Dental (follicular) cyst. This cyst develops from the enamel organ of an unerupted tooth, predominantly the third molar on the lower jaw, the canine tooth and the third molar on the upper jaw. The clinical symptoms of a tooth-containing cyst are similar to those of other jaw cysts, however, when examining the teeth, it is characteristic that one of them is absent in the area where the cyst is located, except in the case of its formation from a supernumerary tooth. The possibility of developing ameloblastoma from a tooth-containing cyst was noted.
X-rays are used to determine the rarefaction of bone tissue with clear, even boundaries, similar to a monocystic lesion, and the presence of an impacted formed tooth, the crown of which either faces into the cyst cavity.
A dental cyst must be differentiated from ameloblastoma and primary odontogenic cyst.
Macroscopically, a single-chamber cavity is determined, lined with a membrane and containing a yellowish transparent liquid with cholesterol crystals.
Microscopically, the cyst shell is represented by a thin layer of connective tissue, covered with stratified squamous epithelium, 2-3 cells thick.
Treatment consists of cystectomy with removal of the impacted tooth or a two-stage operation.
Eruption cyst and gingival cyst. Both cysts are rare. An eruption cyst appears as a limited, small bluish swelling in the area where the tooth is about to erupt and is located above the crown. Microscopically, the cyst shell is lined with non-keratinizing stratified squamous epithelium. Surgical treatment is required only if tooth eruption is delayed.
A gingival cyst develops from the remains of epithelial cells of the gum and has the appearance of a small nodule located in the soft tissues covering the tooth-containing areas of the jaw.
Treatment is usually not required.
Treatment of odontogenic cysts of the jaws. There are two main surgical methods - cystectomy and cystotomy. For a cyst connected to the maxillary sinus, oronasal cystectomy and cystotomy are used simultaneously with maxillary sinus. In addition, there are varieties - plastic cystectomy and two-stage cyst surgery. Indications for their implementation depend on the etiopathogenesis of the cyst, its size and the number of teeth involved in the cyst area
Cystectomy. This is a radical operation in which the cyst shell is completely removed and the wound is sutured. Indications for cystectomy are: 1) a cyst, which is a malformation of the odontogenic epithelium; 2) a small cyst located in the tooth-containing areas of the jaw within 1-2 intact teeth; 3) an extensive cyst of the lower jaw, in which there are no teeth in its area and the base of the jaw is preserved of sufficient thickness (up to 0.5-1 cm), which protects against pathological fracture; 4) a large cyst on the upper jaw, without teeth in this area, with a preserved bone wall of the bottom of the nasal cavity, and also adjacent to the maxillary sinus or pushing it aside without symptoms of sinus inflammation.
It should be emphasized that the purpose of the operation is not only to remove, but also to preserve the teeth that caused the development of the cyst and those adjacent to it. Single-rooted teeth that have caused the development of a root cyst are filled with cement removed beyond the root apex. However, if the cyst is located close to the neck of the tooth, saving the tooth is not advisable, since after resection of the apex and part of the root, the stump cannot withstand the load and quickly becomes loose. A multi-rooted tooth, as a rule, cannot be saved (due to obstruction of the canals), and it is removed. Impacted teeth, which are the cause of the development of a tooth-containing cyst, are removed during surgery in all cases.
Intact teeth that are projected in the cyst area and have a periodontal fissure on the radiograph must necessarily undergo EDI. If there is no reaction to the electric current, appropriate treatment is carried out. The reduced response of the tooth to electric current may return to normal after surgery. If the periodontal fissure is not visible on the radiograph and there is no reaction of the teeth to the current, then before cystectomy the teeth must be depulped and treated.
The operation is performed under conduction and infiltration anesthesia. On the vestibular surface of the alveolar process of the jaw, a mucoperiosteal flap with the base facing the transitional fold is cut out by cutting the mucous membrane to the semi-oval or trapezoidal bone. If there are teeth, the end of the flap should not reach the gingival margin by 0.5-0.7 cm; when removing a tooth at once, the incision passes through its socket. If the cyst is located close to the neck of the tooth, the gingival margin with dentogingival papillae is included in the flap. The size of the flap should be larger than the cyst: it is cut out in such a way that it freely covers the future bone defect and the suture line does not coincide with it. The mucoperiosteal flap is peeled off from the bone with a rasp using a gauze swab. It is placed under a rasp and then the bone above the cyst is exposed. In the absence of bone, care must be taken when peeling the periosteum from the cyst shell. The separated flap is held with hooks or ligatures.
Above the cyst in the projection of the apex of the causative tooth, using a trephine, holes are drilled along the perimeter of the future defect and connected to each other with a fissure bur. The resulting rounded bone plate is removed and the anterior wall of the cyst is exposed. If there is a bone structure, the latter is expanded with nippers or a milling cutter. The size of the bone defect should make it possible to view the cyst and perform resection of the root apex. Using a raspator, an angular elevator and a surgical spoon, the shell of the cyst is peeled off (Fig. 16.8), which easily moves away from the underlying bone, but the connection with the root of the causative tooth remains. To isolate the membrane, the root tip is sawed off to the level of the surrounding bone and the cyst along with the root is removed.
After resection of the apical part of the root at the bone level, it is possible to scrape out the remnants of the membrane in this area, which prevents recurrence of the cyst.
When examining the root stump, it is necessary to determine the presence of cement in the root canal; if it is absent, retrograde filling with amalgam is required. This action prevents inflammation of the bone wound due to infection from the root canal.
After removing the cyst shell, the roots of previously prepared adjacent teeth are exposed, the tips of which are also resected. Then the bone cavity is inspected and the remaining pieces of filling material are removed. The cavity is filled with a blood clot, which is a reliable biological factor in wound healing. Rinsing such a cavity with antiseptics, as well as introducing antibiotics into it, is not indicated. To activate osteogenesis of a large bone cavity, it is advisable to fill it during surgery with a bone graft in the form of crushed stone, flour, etc.
If the flap is reduced, it must be mobilized by linear dissection of the periosteum at the base. The flap is placed in place, the edges of the wound are sutured with knotted sutures made of catgut, sometimes silk. A “mouse” bandage is applied externally to limit the movement of the cheek and lip and create peace in the postoperative area for at least 4-5 days. Painkillers and antihistamines are prescribed, and anti-inflammatory therapy is carried out according to indications. The patient is incapacitated for 6-7 days.
Healing of the bone cavity occurs by organizing a blood clot, as after tooth extraction. In the presence of a large cavity, radiographic examination over a long period of time (up to 1-2 years) reveals an area of clearing, which tends to decrease and subsequently to complete restoration of the bone. If a blood clot becomes infected, an inflammatory process develops. In this case, it is necessary to create an outflow of exudate between the sutures or puncture the cavity outside the suture line and wash it with antiseptic solutions. Daily rinsing for 3-4 days often relieves inflammation. As the purulent process continues, the edges of the wound are pulled apart, washed, and an iodoform tampon is loosely inserted into the cavity, turning the flap inward. As the wound granulates (2-3 weeks), the tampon is forced out, it is gradually trimmed and removed.
Often a cyst developing from the upper second incisor spreads to the palate and leads to resorption of the palatal plate. Isolating a cystic membrane on the palate with large defects (more than 2 cm) is difficult, since the cyst wall is fused directly to the periosteum of the palate. When the cystic membrane is peeled off with a raspatory, ruptures often occur, and therefore removal is carried out in separate parts. Instrumental examination of the oral cavity does not allow distinguishing the cyst shell from the tissues of the mucoperiosteal flap. Leaving sections of the cyst wall always leads to relapse. Therefore, in case of a defect of the palatal plate for more than 2 cm, it is recommended to perform a cystotomy from the side of the palate.
Oronasal cystectomy and oronasal cystotomy. Surgeries are used for cysts that penetrate into the maxillary sinus or push it aside in the case of chronic sinusitis. The essence of the intervention is to connect the maxillary sinus with the cyst cavity and communicate the resulting single cavity with the lower nasal passage. The indication for oronasal cystectomy is the absence of teeth within the cyst or the inclusion of 1-2 teeth in its area. Oronasal cystotomy is used in the presence of a large number of intact teeth facing the cyst cavity, and in patients with concomitant diseases.
The operation is performed under local anesthesia. Dissection of tissue to the bone is carried out 0.5 cm below the transitional fold from the second incisor to the second or third molar. When removing the causative tooth at once, a trapezoidal incision passes through the tooth socket.
As during an operation for sinusitis, the anterior wall of the upper jaw is opened and the cyst is exposed. During oronasal cystectomy, the entire cyst shell is removed, the exposed filled root tips are resected, the cavity is connected to the maxillary sinus, removing the bone bridges between them. Only polyposis-modified areas of the mucous membrane are removed from the sinus, and an anastomosis is created with the lower nasal passage. The operation is completed by suturing the wound of the vestibule of the oral cavity. As a result of the operation, the lower part of the formed cavity ends up with exposed bone walls, which subsequently granulate, scar and partially epithelialize.
During oronasal cystotomy, only the anterior and upper parts of the cyst shell are removed and the apexes of the roots of intact teeth are not resected. As a result of oronasal cystotomy, the lower part of the combined cavity, lined mainly with a cystic membrane, quickly becomes epithelialized.
Like conventional cystectomy, oronasal cystectomy is a radical operation and more traumatic compared to oronasal cystotomy.
"Surgical Dentistry" edited by Robustova T.G.
Fourth edition. Moscow "Medicine" 2010
Clinical examples:
Radicular cysts of the jaws
Neoplasms of the maxillofacial area, including cystic formations
Complications after removal of a dental cyst
After removal of a dental cyst, what unpleasant consequences may be possible? Any surgical intervention using anesthesia, like removal of a cyst, can lead to complications. They arise when the doctor does not fully adhere to the chosen tactics, with incorrect diagnosis at the preparation stage, or with the use of inappropriate equipment. Here at Implantmaster, complications do not arise after cyst removal thanks to the professionalism of doctors, modern equipment and the use of the latest techniques. But every patient should be informed about the likely consequences of the procedure. Body temperature may increase after removal of a dental cyst. Pain in the gum area is possible after removal of a dental cyst. The occurrence of edema and hematomas is inevitable. But their consequences are quickly eliminated by antibacterial drugs and constant cooling compresses. However, there are more serious complications:
- It is necessary to first take a blood clotting test to prevent rupture of blood vessels when accessing the root.
- There is a possibility of injury to nerve bundles. Therefore, the tooth may continue to ache even after the cyst is removed. Taking painkillers helps minimize this effect.
- With poor oral hygiene, suppuration can form again. To prevent this from happening, a course of antimicrobial drugs is prescribed.
- Incomplete removal of the affected tissue leads to secondary infection. It is necessary to check everything carefully before applying stitches.
- Perforation of the walls of the maxillary sinuses. Today this almost never happens.
We are confident of an excellent result, even when other clinics do not undertake cyst treatment. Much also depends on the patient. It is necessary to follow the doctor's recommendations in the first days after surgery. Limit consumption of hot, cold and solid foods. Do not use hard brushes or aggressive chemical rinses, and avoid sports activities. You should take vitamins and NSAIDs. Proper treatment of the body will allow you to return to normal as quickly as possible.
Rehabilitation
The recovery period for soft tissue is up to 2 months, for bone tissue - 5-6 months. The duration depends on the characteristics of the body and compliance with medical recommendations:
- eat soft foods at a comfortable temperature;
- do not eat or drink hot, spicy, salty foods;
- give up alcohol and smoking;
- brush your teeth carefully;
- take all prescribed medications.
Dentists consider cystectomy the most effective and preserving method, which is recommended for everyone in the absence of contraindications.
Where can I remove a dental cyst without extracting a tooth?
If you are concerned about this problem, then we invite you to visit the Implantmaster dental clinic to get rid of a cyst on a tooth by treatment or tooth extraction. For you - qualified specialists, all the necessary ultra-modern equipment and reasonable prices.
The price for removing a dental cyst is determined by the services of an endodontist and a surgeon. Endodontic treatment is required with a microscope, including anesthesia, materials, etc., starts from 6,500 rubles. Removal of the cyst by a surgeon is paid separately—about 10,000 rubles. This cost includes all surgical procedures. Lifetime guarantee for treatment at Implantmaster.
Author:
Stages of performing cystotomy of a jaw cyst
The operation is less complicated than complete removal of the cystic capsule. It is easier, faster, and has a minimum of contraindications. However, after surgery, a defect remains in the mouth, which requires special care.
Progress of the operation:
- pain relief with local anesthetics;
- antiseptic treatment of mucous membranes;
- incision of the gum to the cystic formation;
- removal of the wall, cleansing of pathological fluid inside the capsule;
- suturing the edge of the capsule wall with the edge of the soft tissue;
- treatment with antiseptics and drugs;
- applying a cotton swab soaked in iodine to the wound.
After the procedure, an additional cavity appears, so hygiene procedures must be carried out especially carefully. The doctor prescribes the patient a course of antibiotics and anti-inflammatory drugs.
Over the course of approximately one year, the capsule tissue dissolves and the wound heals. If the tumor was large, the recovery period may take up to two years.
Types of dental cysts
It is customary to distinguish between 2 types of dental cysts - follicular and radicular. Follicular cysts are less common than radicular cysts. In the presence of certain factors, it grows from the dental follicle - the membrane around the growing tooth. When it is large in size and involves adjacent teeth, it is called a follicular dentigerous cyst.
Radicular (odontogenic inflammatory) cysts form on the roots of teeth as a result of pathological processes spreading beyond the root apex. By location, radicular cysts can be apical (root), lateral (lateral), apicolateral and interradicular.
Advantages and disadvantages of jaw cystectomy
| Advantages | Flaws |
|
The price of this manipulation is quite high, but it fully pays for itself by preserving the tooth and eliminating the need for expensive implantation. |