Among the products used during orthodontic correction, orthodontic ring crowns are often found. Despite their less popularity, such designs were invented much earlier than braces. The first devices for correcting malocclusions and dentition were precisely crowns, to the surface of which guide tubes and hooks were attached, which in turn were fastened with rubber rods, which created the pressure necessary to move the teeth. However, the results achieved as a result of the use of such systems were difficult to predict, which led to their imperfection.
The use of crowns was determined by the lack in those days of composite materials that would guarantee a strong connection with the surface of the tooth enamel. Obviously, the “cover” placed over the tooth caused inconvenience to the patient, interfering with the full occlusal closure of the rows. This is what influenced the decision to cut off the upper part of the structure, and led to the appearance of orthodontic rings. For their fixation, not the most reliable types of dental cement were still used, but the absence of obvious interference that made it difficult to perform chewing movements and dock with antagonists was in itself a significant progress.
Over time, products in the form of rings equipped with fastening hooks gave way to traditional braces, in which the power arc is placed in a torque, which allows for precise correction of the position of problem units. Advances in technology have increased the effectiveness of treatment, but rings were still required to secure the brackets to the enamel surface.
Katz bite block
The orthodontic corrector is presented in the form of a removable plate intended for use on the upper jaw. The design consists of a plastic inclined plane and ribbon reversible clasps.
The action of the device is as follows: the lower front teeth are deflected at the moment when they come into contact with the inclined plane, then they are partially immersed in the alveolus.
The use of a Katz plate is indicated when it is necessary to eliminate distal occlusion.
Thus, orthodontic devices are represented by a large number of models, each of which is characterized by its own functions and principles of operation and is aimed at solving problems of any degree of complexity.
Before choosing a device, you must familiarize yourself with all the indications and contraindications for its use in order to prevent the occurrence of severe complications. A wide range allows you to choose the most suitable device in terms of functionality and cost.
Resorption of tooth roots
First of all, it is necessary to talk about the resorption of tooth roots, if we say in general terms - about the resorption of roots. This process has not yet been fully studied and threatens the patient’s complete loss of teeth. Prolonged mechanical impact from the braces system often leads to resorption of the tooth bone tissue. It is very important, at the beginning, middle and at the end of the bite correction, to take diagnostic photographs and look at the condition of the roots, since resorption at the initial stage is completely asymptomatic. Treatment of root resorption is complex, multi-step and expensive. Quite often I hear from patients that a doctor installs a brace system without analyzing an OPTG or CBCT image, without impressions or any diagnostics. This is a gross, dangerous mistake, since the bracket system is not indicated in all cases, and setting it “at random” can lead to unpleasant and often irreversible consequences. Be careful when choosing a specialist.
Advantages of the technique
A properly selected crown, fixed with dental cement, reliably blocks access to the base from the outside. This means that tooth enamel is protected from pathogenic bacteria and microbes that provoke the development of caries and other diseases. In addition, dentists note a number of positive aspects, including:
- Reducing the duration of correction due to the absence of the likelihood of individual braces coming off;
- Easy to maintain oral hygiene;
- Ability to use extraoral appliances, including a facebow.
After completion of orthodontic treatment, the orthodontic ring is removed, and the patient is given a date to visit an orthopedic dentist to make an artificial crown for the already treated tooth.
Advantages and disadvantages
The indisputable advantage of an orthodontic ring is the ability to install it on fixed dentures or implants, as well as on a significantly damaged coronal part of the tooth. Braces cannot be attached to an artificial crown or implanted tooth, so rings are a solution to the problem.
Other advantages of orthodontic rings with braces:
- there is no need to remove “extra” healthy teeth, which is especially important in case of overcrowding;
- during the installation process and after it, the mucous membranes of the mouth are not injured, making adaptation to the system much easier;
- the ultra-thin product easily fits into the interdental spaces and is easily placed in the right place;
- Before installation, the doctor administers anesthesia, so there is no pain, only mild discomfort is possible;
- The size of the gaps formed between the teeth is strictly controlled.
Flaws:
- preparing and fixing the bandage takes quite a lot of time and is done over several visits to the doctor;
- the risk of accumulation of food plaque on a “ringed” tooth increases;
- sometimes complications arise in the form of increased tooth sensitivity, gum inflammation and pulp necrosis - death of the neurovascular bundle;
- the likelihood of demineralization of tooth enamel increases.
What is it used for?
Orthodontic rings for teeth are placed in case of severe malocclusions, when increased reliability of fixation is required. They stay on the teeth much better than braces, which allows you to slightly expand your diet. But the main thing is that when the bracket comes off or chips, the healing process is actually interrupted, and as a result, the correction takes more time.
Rings are installed only according to indications, so they are not installed unless necessary. The exception is when braces often come off or are damaged mechanically. An orthodontic ring will add additional strength to the brace system and reduce the risk of breakage.
Important!
Iron bands are placed in posterior teeth due to excellent visual access. That is, if caries or other diseases develop, the doctor will see this, which cannot be said about incisors or canines. It is impossible to determine that the tooth has begun to decay until the metal ring is removed. This is precisely its main drawback.
Interdisciplinary reception
It often happens that malocclusions are much more complex and treatment with braces alone is not enough.
Often, treatment, for one reason or another, is delayed or does not go according to plan, or is initially planned incorrectly, which creates a lot of problems physically and psychologically for both the patient and the doctor. Therefore, I strongly recommend that you undergo a detailed diagnosis before orthodontic treatment. Calculation of casts, images, CBCT analysis, determination of central occlusion and central relationship of the jaws. According to the indications, axiography. This will allow you to make an accurate diagnosis. Accurate diagnosis = correct treatment plan. The orthodontist must have the skill, knowledge and ability to conduct interdisciplinary treatment. Your treatment will be monitored simultaneously by the orthodontist and related professionals: orthopedist, surgeon, gnathologist, periodontist, therapist, endodontist, and, if necessary, an osteopath. If necessary, during orthodontic treatment, a competent orthodontist with interdisciplinary experience will attract the necessary specialists to provide timely assistance. This work in conjunction allows you to speed up treatment and avoid complications. Treat previously undetected caries in a timely manner, rather than wait for further tooth destruction under braces until removal. Or, for example, if there are periodontal problems, then your doctor will treat in accordance with the treatment protocols of the periodontist, constantly communicating with each other.
Patients with TMJ disease must first undergo a full diagnostic with axiography, and, if necessary, therapeutic and diagnostic splint therapy from a gnathologist. This therapy allows you to put the joint in the correct position. This correct position may not seem entirely comfortable to the patient; the teeth may touch at completely different points than before. But it is only from this functional position (in case of TMJ pathology) that it is possible to begin orthodontic treatment, so that incorrect movements do not cause more harm to an already suffering person.
Ainsworth's device
Mechanical orthodontic device.
general characteristics
It is a non-removable arc device. The design includes rings or crowns, a tangent wire, vertical tubes that perform a supporting function, and a spring arch.
Operating principle
The main role in this device is given to the arc. It is bent in such a way as to follow the line of the dentition.
The action of the design is based on the tendency of the arch to its original shape, as a result of which all the teeth attached to the components of the device shift behind it. The strength is adjusted by a doctor.
Indications for installation
"Ainsworth" has versatility in application and can be used to solve most problems associated with bite.
Manufacturing and fastening process
The manufacturing procedure is based on a number of steps:
- preparing a plaster cast of the jaw;
- making a plaster model, tubes and wire;
- fitting, finishing and connecting elements, their installation on a plaster model;
- arc manufacturing;
- installation of the finished structure.
Before installing the device, you need to remove plaque and tartar.
Therapy process
For treatment to be effective, you must follow all the requirements and recommendations of the doctor.
The duration of the adaptation period ranges from 1 week to 1 month. At this time, it is important not to eat foods that contribute to painful sensations, to carefully care for the oral cavity, to use soothing and disinfecting decoctions, painkillers prescribed by a doctor.
In addition, you need to be monitored by a doctor approximately once a week.
Advantages and disadvantages
The Ainsworth arc is characterized by reliability, individual model for each patient, guaranteed results, constant medical supervision, and variability of action.
The disadvantages of using it are that the device is quite noticeable, requires a long time to get used to, complex care, a long preparation process, and the possibility of a doctor making a mistake cannot be ruled out.
Quite effective in correcting most dental pathologies. Has precise impact.
Treatment price
The cost of installation, services for weekly monitoring and subsequent removal averages from 10 to 15 thousand rubles.
Herbst's proofreader
Refers to non-removable orthocorrectors.
general characteristics
The Herbst apparatus has a complex design. The main purpose is to correct severe malocclusions.
The orthosystem consists of supporting crowns and two hinged beams.
Operating principle
The action of the device is based on the fact that the lower jaw is gradually moved forward as a result of its constant forced tension. It is characterized by the speed of action.
Indications for installation
Designed for the treatment of first class distal occlusion.
Preparation and fastening
Before installation, detailed preparation of the teeth is necessary. It is necessary to cure problematic molars, replace old and unreliable fillings.
Then comes the stage of taking impressions of the jaws and sending them to craftsmen to make the device.
Treatment process
The orthodevice has a constant, continuous effect, contributing to the achievement of a guaranteed, positive and fairly quick result, the ability to accurately predict the results of use, and rapid addiction.
The main disadvantages are the presence of bulkiness and poor aesthetics.
Price
The final cost of the device is influenced by its type. Therefore, the price can vary from 4,500 to 30,000 rubles.
Functional
By function, such devices can be divided into:
- Distalizing
. If the baby tooth was removed too early, and the permanent one managed to move forward and take its place, so-called “distalization” is required - moving the tooth back. As a result of this process, we are able to create space for all the permanent teeth without resorting to permanent tooth extraction or separation. For distalization, devices such as Pendulum, Pendex, Distal Jet, etc. are used. - Expanding
. Expansion during the period of primary and mixed dentition occurs as efficiently as possible - since the impact extends not only to the teeth, but also to the jaw itself (a skeletal effect is achieved). At the age of 6-11 years (and sometimes later), the maturation of the bone sutures has not yet been completed and this age is considered the most favorable for obtaining true expansion of the upper jaw.
Design features
The advisability of using seemingly outdated rings or crowns is determined by the significant loads placed on the molars. Practice shows that a well-chosen and well-fixed ring can withstand greater pressure than a composite. However, in order to install rings on the chewing elements, you will need to visit your dentist at least twice.
During the first session, separation rings are used, thanks to which the doctor is able to create minimal gaps between the units, sufficient to place orthodontic crowns. The restoration technique does not involve preparation of the enamel, so the teeth are moved apart in the traditional mechanical way - using rings made of elastic material.
Inserted into the gap between the teeth, the ring initially contracts, but as it is worn, it gradually restores its original shape, simultaneously moving the teeth apart. The gap sufficient for placing an orthodontic ring is considered to be 0.2 mm, which can be achieved in just 5-7 days of wearing the sliding element. The design involves applying small serrations to the inner side of the ring, which improve the connection with the adhesive composition, while on the outer rim there is a bracket equipped with two grooves and a hook. The use of markings allows models to be quickly matched to the specific teeth for which they were designed.
Product of Derichsweiler or Nord
The Derichsweiler apparatus is a non-removable screw orthodontic system that has a mechanical effect. Its design includes a plate in which crowns or rings are secured, and a screw.
In some cases, various springs and levers are also included in the design.
Preparatory stage and installation
The manufacturing process includes the following steps:
- obtaining a plaster model of the jaw;
- production of supporting elements;
- checking and taking impressions;
- re-production of a plaster model based on an impression;
- modeling of the palatal base, strengthening of metal reinforcement and screw;
- installation.
It is highly effective in the treatment of certain pathologies.
Space holder for children's bite: types and designs
Pediatric orthodontists at Aza&Buka dentistry select a tooth space holder based on the specific clinical situation. Main options:
Replacement plate - a plate with artificial teeth to replace missing milk units. Completely restores the functions of the jaw row, maintains the bite, and helps the permanent units to erupt in a timely manner due to the correct pressure on the bone tissue. Replacement plates are adjusted to suit the child’s changing bite - as the jaw grows, until the appearance of missing permanent teeth. The product is removable and is attached with metal or plastic hooks to adjacent teeth.- A two-jaw removable functional appliance is a design for solving several orthodontic problems. Artificial teeth replace the removed units, and the relative position of the dental arches is responsible for the harmonious overlap of the lower teeth with the upper ones.
- A place retainer is a non-removable orthodontic product. A rigid metal ring fences off the area where the permanent tooth will erupt and prevents the mobility of neighboring units. Once the molar begins to grow, the holder is removed, allowing the permanent unit to take its place. The design is excellent for replacing a first or second molar. It is placed mainly in “invisible” zones.
Fixing elements of orthodontic devices
Golovko Nonna Vasilievna , Associate Professor of the Department of Propaedeutics, Orthopedic Dentistry and Orthodontics of the Ukrainian Medical Dental Academy.
Fixation is the strengthening of the orthodontic apparatus or denture on the jaw in static conditions, and stabilization is the stability of the orthodontic apparatus or denture during functions (speech, chewing, swallowing).
One of the most common methods of fixing removable orthodontic appliances and dentures is the use of fixing devices, which include:
- Clasps.
- Crowns or rings.
- Mouthguards.
- Combined fixation according to M.A. Napadov (dentoalveolar or dentogingival).
A clasp (from German – klammer – hook) is a special device that is designed for attaching the base of a removable orthodontic appliance or denture to the teeth.
Clasps are classified as follows:
I. By location: dental, gingival (pelota), dentogingival;
- Clasps using the subequator tooth space: - single-arm round bent clasp,
- - Jackson flip clasp,
- - Duisings clasp,
- - Adams clasp,
- - frame clasp,
- - tape clasp.
- - Schwartz arrow-shaped clasp,
II. According to the nature of contact between the clasp arm and the tooth crown:
- Group 1 – clasps with a plane contact of the shoulder to the tooth crown (bent and cast tape clasps). Clasps of this group have a large surface of contact with the crown of the tooth and sometimes lead to abrasion of the enamel and make it difficult for the teeth to self-clean from food debris, which can lead to the development of caries. They are also imperfect from an aesthetic point of view. The fixing effect is achieved by increasing the plane of contact of the clasp arm to the tooth and the force of its pressing. However, the latter increases the load on the supporting tooth.
- Group 2 – clasps with a linear contact of the shoulder to the tooth crown. This group consists of the following clasps: round single-arm bent clasp, Jackson flip clasp, Duisings clasp, frame clasp and others. Such clasps have sufficient elasticity because they are bent from round elastic orthodontic wire. The improvement in the fixing effect in the Jackson reversible clasp and the Duisings clasp in comparison with the round single-arm bent one is explained by the increase in the area of contact between the shoulder and the body of the clasp to the tooth. They are less noticeable to others.
- Group 3 – clasps with a point contact to the tooth crown. This group consists of the following clasps: button, spear-shaped, hook-shaped, arrow-shaped Schwartz and Adams clasp. They have greater elasticity because they are bent from thinner orthodontic wire. These clasp designs optimally solve basic problems and provide fixation of removable orthodontic appliances and dentures. They are hardly noticeable.
In comparison with clasps of groups 1 and 2, clasps of group 3 minimally injure the tooth enamel, since they contact the tooth surface pointwise, that is, over a small area.
III. Shape: (round, semicircular, flat or ribbon).
IV. By manufacturing method: (bent and cast).
V. According to the degree of coverage of a tooth or several teeth: (single-armed, double-armed, ring-shaped or reversible, double and multi-linked).
VI. By function: (retaining and support-retaining). Retaining clasps are intended exclusively for fixing removable orthodontic appliances and dentures. With these types of clasp fixation, the vertical chewing load is completely transmitted through the base to the mucous membrane. Support-retaining clasps of clasp dentures and orthodontic clasp appliances not only fix, but also make it possible to distribute the chewing load between the mucous membrane of the prosthetic bed and the periodontium of the supporting teeth.
VII. According to the material from which the clasps are made: steel, gold, plastic.
VIII. According to the method of connection with the base or in relation to the body and shoulder of the clasp: rigid or stable, springy or semi-labile, articular or labile.
IX. Depending on the number of teeth used for fixation: point fixation - use of 1 single-arm clasp, linear - use of two single-arm clasps, planar - use of more than 3 single-arm clasps.
Retaining clasps, which are most widely used in orthodontic practice, consist of a shoulder, a body and a process.
The clasp arm is its elastic part, which covers the crown of the abutment tooth. Its location is determined by the anatomical shape of the tooth. In practical dentistry, it is customary to divide the surface of the tooth crown into 2 parts: occlusal and cervical. The boundary between them is the equator, that is, the line that runs along the most convex part of the tooth. The clasp arm provides fixation of a removable orthodontic appliance or denture. Crossing the belt of the supporting tooth, it is tightly pressed against the gingival part, which has the smallest diameter.
When making the arm of a retaining clasp, you must remember the following requirements:
- The shoulder should cover the tooth from the labial or buccal side, located directly behind the line of greatest convexity, that is, between the equator and the gum.
- The clasp arm, round or flat, should touch the tooth surface at as many points as possible. The fit at only one point leads to a sharp increase in pressure during movements of the base of the prosthesis or apparatus and leads to abrasion of the enamel.
- The shoulder should be elastic when the base shifts. Not all clasps have this quality. Wire clasps are the most elastic, cast ones are less flexible. Unlike bent wire clasps, cast clasps more accurately follow the relief of the tooth surface.
- The shoulder should be passive, that is, not transfer pressure to the supporting tooth.
- The shoulder must be rounded and polished to prevent injury to the buccal mucosa.
The clasp body is its stationary part, which is located above the equator of the abutment tooth on its contact side. It should not be placed below the equator (near the neck of the tooth), since in such cases the clasp interferes with the application of the prosthesis or orthodontic apparatus. On the front teeth, from an aesthetic point of view, this rule can be abandoned by placing the body of the clasp closer to the gingival margin.
The clasp extension is designed for attaching the clasp to the base of a prosthesis or orthodontic apparatus. It should be 0.5-0.7 mm away from the mucous membrane.
The clasps are placed in the orthodontic appliance or denture in such a way that they do not interfere with the rotation of the base.
Clasp fixation is called point fixation if it is located in one area (on one tooth). Fixation in which the clasps can be connected by a line is called linear. The location of the clasps at three or more points allows them to be combined along a plane, which is why such fixation is called planar. This type of fixation is more reliable. The reliability of fixation depends not only on the number of clasp points, but also on their relative position in relation to the midline of the alveolar arch. The conditional line that connects 2 clasps is called a clasp line. It can cross the midline of the alveolar process at an angle that is close to straight; cross it diagonally or run parallel to it on one or both sides. Thus, clasp lines can have a transversal, diagonal or sagittal direction.
To fix a removable orthodontic appliance or prosthesis on the lower jaw, it is advisable to place the clasps along the transversal, as they will counterbalance the lifting of the base by the muscles of the tongue and floor of the mouth.
To fix a removable orthodontic appliance or prosthesis on the upper jaw, it is better to use a diagonal arrangement of clasps, since the diagonal clasp line crosses the midline of the alveolar process and the fixing effect of the clasps extends to both halves of the prosthesis.
The choice of fixing elements depends on:
- presence of teeth and interdental contacts,
- group affiliation of the tooth,
- tooth crown height,
- expressiveness of the equator,
- presence (severity) of the vestibular subequatorial space,
- depth of the vestibule of the oral cavity,
- the presence of space between the upper and lower teeth in a state of central occlusion.
Single-arm round bent clasp:
It is the easiest to manufacture and ensures good stability of the apparatus if it is placed taking into account the direction of the acting forces and is manufactured in sufficient quantity. The choice of abutment teeth is associated with the location of the clasp lines.
Place a single-arm round curved clasp on the lateral teeth (2-3 on each side of the dentition). It is bent from orthodontic wire with a diameter of 0.6-0.8 mm (0.6 mm wire for temporary teeth, and 0.8 mm for permanent teeth). It covers the tooth in the subequatorial space. If it is made on the last distally located tooth, then it should not cross the interdental occlusal space.
A single-arm round bent clasp consists of a shoulder that covers the tooth from the vestibular side; body - the middle, or elastic part, which connects the clasp arm with the process and the process, which is welded into the base of the orthodontic apparatus or denture.
Such a clasp covers the tooth only on one side and performs only the function of holding. Since the clasp is firmly fixed in the base, its shoulder has a constant elastic action.
The clasp on the tooth is placed strictly in relation to the equator. On the teeth of the upper jaw, the clasp arm is located above the equator, on the teeth of the lower jaw - below, which ensures that the arm slides along the convexity of the tooth crown when fixing the apparatus. The height of the clasp should be determined taking into account the closure of the dentition so that it does not interfere with the movements of the lower jaw. The larger the elastic part of the clasp, the more elastic it is and the less harmful the effect it has on the supporting tooth.
A single-arm round bent clasp can be made elongated and cover the tooth located in front. But this does not lead to a significant improvement in the retention effect.
If it is necessary to use both a plate apparatus and rings on molars with locks and tubes to fix extraoral traction, a single-arm clasp is located under the lock and tube.
If there are defects in the dentition, it is possible to manufacture a round, double-armed clasp, in which one arm covers the tooth from the vestibular surface, and the other from the oral surface. Both shoulders are united using a body, which is placed in the area of the defect. It is advisable to use such a clasp design in the manufacture of removable orthodontic appliances, which also perform the function of replacing dentition defects.
Such a clasp can be bent from one piece of wire with a diameter of 0.6 mm or made up of two single-arm clasps.
Ear-shaped clasp - also bent according to the principle of making a single-arm round bent clasp, but at the end of the shoulder there is a curve in the form of an auricle. The ear-shaped clasp can be made multi-link.
The Jackson flip-over clasp has two bodies and two branches. This type of clasp is called combined due to the creation of elements of resistance and the transfer of pressure to the crowns of the teeth. To make a clasp, orthodontic wire with a diameter of 0.8-1.0 mm is used.
The Duisings clasp (Fig. 17) has 2 semicircular bends on the shoulder, which enhances its elasticity, elastic properties and fixation. For its manufacture, orthodontic wire with a diameter of 0.5-0.6 mm is used.
A necessary condition for using the Duisings clasp is a sufficient height of the crowns of permanent teeth.
Rice. 17. Duisings clasp.
The frame clasp differs from the designs described above in that its shoulder covers a group of teeth. The retaining part – the frame – is placed on the vestibular surface of the lateral teeth. It presses the teeth against the base of the apparatus and does not slide on the latter, since the equator of the supporting teeth prevents this. The part of the frame that is located in the area of the alveolar process should lag behind the mucous membrane by 0.5 mm and not reach the transitional fold.
Frame clasps are indicated during the period of teeth change. The loss of a temporary tooth does not weaken the fixation of the device, since the clasp rests on several teeth. Frame clasps are convenient in cases where the equator of primary teeth is well defined.
Tape clasps are rarely used in the manufacture of orthodontic structures, mainly for retention of the location of anterior teeth after their rotation around an axis or mesio-distal movement. In the latter case, the clasp on the vestibular surface of the tooth is shortened and left in the form of a barely noticeable paw. To make a tape clasp, use a flat steel tape 1.5-2 mm wide and 0.3-0.4 mm thick. It can also be made from round orthodontic wire with a diameter of 0.9-1.0 mm, if it is flattened using rollers or a hammer. The clasp is placed between the teeth, so in some cases it is necessary to engrave plaster teeth on the model.
Button clasp - made from standard orthodontic wire blanks with a diameter of 0.6 to 1.0 mm, at the end of which there is a drop-shaped extension. It is used in the presence of tight contacts of adjacent teeth. The button (drop), that is, the holding part of the clasp, is placed between the teeth (Fig. 20.1).
Rice. 20. Button clasp – 1, spear-shaped and diamond-shaped (frame) clasp – 2.
Spear-shaped clasp - also made from standard orthodontic wire blanks with a diameter of 0.7 mm, at the end of which there is a spear-shaped thickening. The clasp provides reliable fixation of the orthodontic apparatus (Fig. 20.2).
The Schwartz arrow-shaped clasp is made as one- or two-link. It is bent from orthodontic wire with a diameter of 0.6 mm. It is quite elastic and fits well into the interdental spaces (Fig. 21.1)
Rice. 21. Schwartz arrow-shaped clasp.
It is possible to manufacture a multi-link arrow-shaped Schwartz clasp (Fig. 21.2). First, the arrows are bent, their shoulders are connected, and then the body and shoots are made. If the use of an intermaxillary rubber traction is indicated, then on the medial shoulder the hook is bent, directed forward, and on the distal shoulder, backward. It is possible to connect arrow-shaped clasps with periodontal pads.
Triangular double-arm clasp - similar to the Schwartz clasp, but more convenient to manufacture. In this case, the arrow-shaped part is replaced with a triangular one.
The Adams clasp is the most versatile and effective. It is used both on single teeth and on teeth that are located in the dentition. This clasp belongs to the group of clasps with a point contact of the shoulder to the surface of the tooth crown. This arrangement of the clasp on the vestibular surface of the tooth crown in its cervical area ensures reliable fixation of the device. Clasps press the teeth against the base of the orthodontic apparatus and prevent the abutment teeth from deflecting and rotating around their axis. They are placed on the first temporary molars or premolars and the first permanent molars.
The body of the clasp should be located above the contact point in the recess between adjacent teeth, crossing the dentition. There are several types of Adams clasps: single, with one fixing protrusion, double (usually made for central incisors, with a hook for intermaxillary traction, with soldered horizontal tubes for the face bow, with processes, etc.
Loop-shaped clasp - made in the same way as a regular round bent clasp, but one loop measuring 3-4 mm is made at the end of the arm.
Triangular clasp - its fixing edge has a triangular shape with sides 5 mm long, converging at an angle of 600 (Fig. 23).
Rice. 23. Triangular clasp
Other types of fixation
Dentoalveolar or dentogingival fixation according to M.A. Napadovu is combined, as it consists of a wire frame and plastic shields located on the alveolar processes.
Fixation according to M.A. It is convenient for Napadov because various auxiliary elements can be placed in plastic pelots (hooks for traction, tubes for the Engle sliding arc, tubes for the face arc, etc.); it holds and stabilizes the orthodontic apparatus based on the teeth and alveolar processes.
Difficulties in applying the device with fixation according to M.A. Napadova occur in the presence of teeth with a well-defined equator.
Mouthguards made of plastic or metal are also used as fixing elements. Such a mouthguard should cover the crowns of the supporting teeth, but not injure the gingival margin and interdental papillae.
Plastic mouth guards. More often, two temporary molars on each side of the jaw are covered with a mouthguard. The thickness of the mouthguard on the occlusal surface should ensure separation of the bite on the front teeth with the elimination of their reverse overlap in the case of a mesial bite, or be equal to 2-3 mm in case of an open bite.
Metal mouthguards. If a mouth guard is needed for a larger number of teeth, it can be made from individual links (3-4 teeth each) and connected by soldering. According to indications, the mouthguard can be made from metal alloys by casting.
Crowns are widely used for fixation of fixed orthodontic appliances, as well as for bite separation. Orthodontic crowns are made from ordinary or thin-walled metal sleeves (0.15-0.18 mm thick) according to generally accepted rules.
, rings are used more often than metal crowns. They do not separate the bite, allow you to monitor the condition of the teeth being moved, and are also more aesthetically pleasing and easier to remove than crowns. Recently, standard ring blanks have been used more often. Locking devices, tubes of different diameters and different cross-sectional shapes, stops, etc. are welded to the rings.
Basic rules for fixing separating rings
To securely fix the separating rings on the teeth, it is necessary to adhere to some rules, namely:
- It is necessary to maintain a certain interval between the occlusal edge of the molar and the middle line of the lock groove. For the 1st upper molar it should be 4 mm.
- The lower edge of the bandage and the chewing surface of the molar should be parallel.
- There should be no obstacles to the teeth closing.
You can buy separation rings to correct your bite on our website. Also, it is worth noting that delivery of separation rings throughout Moscow is absolutely free, but provided that the order amount is more than 5 thousand rubles. This is possible when purchasing separation rings in bulk, or in addition to other orthodontic products.
Historical reference
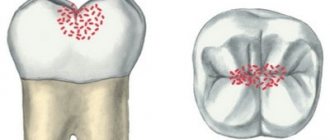
The most recognizable device used in orthodontics is braces. However, few people know that separation rings were actively used by dentists back in the first half of the 20th century - before the invention of metal brackets, which are familiar to most patients today who had to correct malocclusions or abnormalities in the development of the jaw. In fact, the rings performed a similar task - they created constant pressure on molars and premolars growing in an unnatural anatomical position, and forced them to take the correct position.
Technically, the first separation products were more like metal crowns, the dimensions of which could be changed using a built-in screw. The devices also included guide clasps and tubes through which an elastic rod was passed, providing the necessary force. The main drawback of the design is the inability to predict the result and control the dynamics of changes during the treatment process, so the outcome of the correction was often even worse than the initial situation.
However, everything changed with the discovery of technology that makes it possible to produce crowns that exactly copy the structure of the tooth on which they were installed. From this moment on, doctors could form permanent correctors by securing them with forceps and soldering the seam from the inside of the row. Obviously, the procedure was not very comfortable for patients - however, an alternative had to wait for some time, until the advent of composites. But the main idea was to remove the upper part of the corrective crowns, as a result of which their shape began to resemble a ring.
Why do patients trust Aza&Buka dentistry?
When carrying out orthodontic treatment, Aza&Buka Pediatric Dentistry focuses on the most modern protocols and selects correction methods that are optimal for the child. For patients and their parents this means:
- Professionalism of doctors. Pediatric orthodontists will conduct a full diagnosis, explain whether a plate is placed on baby teeth if only one unit is missing, and choose the optimal treatment regimen to preserve the bite.
- Making the device from casts. To ensure that the space retainer accurately matches the child's bite, the doctor will take impressions, create a plaster model, and order a dental laboratory to make a replacement plate exactly for the child's baby teeth.
- The ability to find an approach to each child. Removable orthodontic plates are prescribed to be worn almost constantly. Children often sabotage this moment. After communicating with Aza&Buka orthodontists, the children themselves ensure that the plate is in their mouth - they do not become capricious and do not argue with their parents.
How is the appointment going?
Plates with artificial teeth for children are produced in several stages:
- Examination by a pediatric orthodontist
The doctor will evaluate the condition of the teeth, the characteristics of the bite, and the prospects for the eruption of the molars. He will refer you for a detailed examination - x-ray, optg.
- Preparing the child's mouth
Before the manufacture and installation of an orthodontic holder, the baby’s teeth will be treated and impressions will be taken to prepare a replacement structure.
- Making and installing a record
When fixing the product in the oral cavity, doctors focus on the convenience and comfort of the young patient. The seat retainer should not rub the gums or interfere with speech or eating.
- Care training and questions answered
An orthodontic replacement plate requires systematic cleaning, which the doctor will tell the child and his parents about. The specialist will also answer all questions about the duration and importance of treatment.