.
In medicine, an enlarged child’s tongue is called “macroglossia.” This disease is associated with structural abnormalities both on the surface and inside the tongue. A very large tongue can be observed mainly in children; in adults, macroglossia occurs with a frequency of 1–2%.
A doctor can diagnose macroglossia both if the tongue is completely enlarged, and if its individual parts are swollen - the back, tip, side.
Macroglossia of the tongue can be a congenital or acquired disease
What does tongue position affect?
Language takes part in many important processes:
- determines the taste and temperature of food;
- helps in mixing food and saliva, starting the digestion process;
- facilitates swallowing;
- participates in the formation of speech.
And also, making several thousand movements per day (swallowing movements alone are about 2000), the tongue participates in the formation of the arch of the palate and bite.
The relationship of the jaws in the bite has a close relationship with the position of the head relative to the body and posture in general.
Bite is the relationship between the dentition of the upper and lower jaws during their tight closure. Depending on age, the bite can be milky, replaceable or permanent. Classification of occlusion is not the topic of this article, so I will focus only on the description of physiological occlusion, which is characterized by the following features:
- does not interfere with the process of eating;
- does not distort speech;
- does not spoil the external characteristics of the face.
When the teeth are completely closed, the physiological occlusion meets the following indicators:
- the upper dentition covers a third of the lower dentition;
- all opposing chewing teeth of the upper and lower jaws fit well together;
- a conventional central line drawn vertically along the face divides the jaws into equal halves.
I apologize in advance to orthodontists for such a simplified description of the physiological bite and there may be some other inaccuracies. I hope the meaning of the article did not suffer from this.
For proper growth of teeth, the so-called myodynamic balance must be formed in the oral cavity, that is, the pressure of the tongue from the inside on the dentition of the upper jaw must correspond to the pressure of the muscles of the lips and cheeks from the outside.
Normally, the tip of the tongue is in a neutral position, located behind the upper incisors, without touching them. Where the tongue is when we pronounce the sound “H” is the so-called “resting point”. During each swallowing movement, the back of the tongue is pressed against the palate, stimulating the growth of the upper jaw in width, improving blood supply to the nasal and oropharynx and thus increasing local immunity. The correct position of the tongue at rest and when swallowing is only possible with nasal breathing, while the mouth must be closed. When breathing through the nose, all the air inhaled has time to be purified and warmed up. The air flow passing through the nasal turbinates also stimulates the growth of the upper jaw in width and the harmonious growth of the entire middle third of the face.
Now I will dwell a little on the changeable bite and the problems of the formation of a physiological bite, which become obvious precisely during the change of teeth. Usually this age ranges from 4-5 years to 12-14 years. During the mixed bite, the most intensive growth of the jaw bones occurs, so bite correction is also most effective at this time.
In children who breathe through their mouth, the so-called “adenoid” type of face is formed, the face becomes narrow and long - elongated. Narrow jaws cause a lack of space for permanent teeth, that is, they are crowded. The Gothic palate and lack of space for the back of the tongue creates problems with sound pronunciation.
Children with malocclusion often breathe through their mouths, even if the nasal passages are clear. They develop habitual mouth breathing and begin to get colds more often. It has been proven that mouth breathing reduces blood oxygenation, as well as the transfer of oxygen to tissues. The brain suffers more than other organs from hypoxia. Children become irritable, not assiduous, and not attentive.
The tongue in such children is in the middle (interdental) or low position - between the palate and the lower jaw. When swallowing, it does not rest against the roof of the mouth, but against the teeth. The tongue is a powerful muscular organ and when it is pressed, the teeth deviate from their normal position.
Very often this is combined with weakness of the orbicularis oris muscle, which normally should balance the pressure on the teeth from the outside.
Normally, swallowing should be visible only by the movement of the thyroid cartilage, the face should not tense. If the position of the tongue is incorrect and the orbicularis oris muscle is weak, the child has to use additional muscles to keep the mouth closed when swallowing. He begins to help himself when swallowing with the corners of his lips, facial muscles, neck movements, shoulders, and sometimes even his stomach.
The tongue, in the middle or lower position, blocks the airways and, in order to somehow open them, the child is forced to move his head forward and raise his chin. This unnatural position of the head and neck also changes the upper chest. Orthopedists, seeing such a picture, talk about poor posture.
So, a change in the position of the tongue leads to a change in the position of the head, a distortion of the anatomically correct location relative to each other of the cervical vertebrae, hyoid bone, cartilage of the larynx and soft tissues of the neck, trachea and esophagus, vessels supplying the brain, and nerve trunks that ensure the functioning of all internal organs.
Thus, during a mixed dentition, it becomes extremely important to form nasal breathing and create conditions for the anatomically correct position and functioning of the tongue, because this will contribute to both the normal development of the dentofacial system and the child’s entire body.
- normal chewing, facilitates the functioning of the entire gastrointestinal tract;
- normal swallowing forms a correct bite and harmonious facial features;
- nasal breathing reduces the risk of colds (the air is purified, warmed, lymphoid tissue is not subject to additional stress and does not hypertrophy);
- improves central nervous system function due to sufficient oxygen supply;
- communication function improves due to clear and understandable speech;
- Due to correct posture, a sense of balance, dexterity, and coordination develops.
Correct bite and anatomical position of the tongue are the key to the health and well-being of your child.
I would like to briefly list the factors that can lead to incorrect position and functioning of the tongue:
- Intrauterine factors (multiple pregnancy, abnormalities in the structure of the uterus, increased tone of the uterus during pregnancy, genetic conditions, etc.);
- Traumatic childbirth;
- Prematurity;
- Artificial ventilation in the first year of life;
- Artificial feeding;
- Untimely introduction of complementary foods;
- Lack of solid food in the child’s diet;
- Bad habits: thumb, tongue, cheek, and various objects sucking, prolonged pacifier sucking (more than 1.5 years);
- Premature loss of baby teeth;
- Frequent diseases of the ENT organs, enlarged adenoids.
What causes the disease
Doctors divide the etymology of the disease into two categories: congenital and acquired.
The congenital form develops with intrauterine developmental disorders of the fetus. Abnormalities in a child in the womb can be affected by various factors, so a single cause could not be determined.
Scientific definition of macroglossia
Macroglossia develops independently against the background of:
- Down syndrome;
- open or malocclusion;
- tuberculosis;
- hormonal imbalance, as well as syphilis;
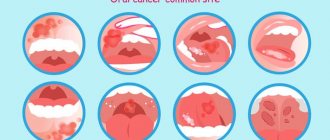
- infectious diseases that affect the tongue;
- poor circulation or hemorrhages in the oral cavity;
- tongue abscess - death of its tissues; various forms of glossitis (catarrhal, candidal) - enlargement of the nipples of the tongue;
- bruises and injuries, tumors, cysts that affect the circulatory system of the tongue and surrounding tissues, as well as lymph nodes;
- when pus accumulates in the oral cavity - under or above the tongue; and also if the muscles of the tongue are very large - abnormal development;
- acromegaly; myxedema; acute allergic reaction syndrome;
- actinomycosis of the tongue.
Down syndrome is often accompanied by varying degrees of enlarged tongue
Glossitis, as a factor contributing to the enlargement of the oral organ, can be provoked by:
- an abundance of harmful bacteria - viruses found on the tongue;
- scalding with hot food/drinks, poor diet, excessive indulgence in sweets;
- poor dental care, incorrectly selected balm and mouthwash;
- injuries, cuts, chemical burns of tongue tissue.
What parents should pay attention to and be wary of
- Breathing through the mouth if the child does not have a runny nose.
- No gaps between teeth by 4-5 years.
Baby teeth are small and there is usually always room for them, even if the jaw has not developed enough. As the child grows up and prepares for a mixed dentition, so-called trema should appear between the baby teeth - small but distinct distances. When baby teeth fall out, permanent teeth will erupt, which are much wider than baby teeth, and they should have enough space for normal growth and the formation of an even, beautiful dentition.
- Observe the child’s swallowing of saliva; normally, swallowing occurs imperceptibly, without tension in the facial muscles.
Usually, during an appointment, a pediatric dentist draws the attention of parents to the emerging problems of forming a correct bite and refers such children to an orthodontist.
If this does not happen, it is necessary to show the child at the age of 4-5 years to a pediatric orthodontist, preferably one who takes into account the functional approach in his work.
Therapeutic effect
When choosing the type of therapy, the doctor takes into account the form of the disease and the cause of its origin. If this pathology is caused by a secondary disease, the cause should be treated in parallel. The general treatment algorithm involves the use of the following medications:
- antibacterial drugs that are used orally or injected;
- antiseptic solutions that are used for local treatment of the surface of the muscular organ;
- the use of anti-inflammatory drugs for treating the tongue.
When treating the main disease that caused macroglossia, with an integrated approach, medications have a positive effect on the organ, it gradually becomes smaller in size. The therapy is long-term, the duration of the course of taking medications is determined by the treating doctor. It is also necessary to undergo regular examinations, since treatment adjustments may be necessary as the patient recovers.
How to correct malocclusion and tongue position.
There must be an integrated approach. Modern orthodontics offers various ways to straighten teeth. But as we have already seen, straightening teeth is ineffective without eliminating the causes leading to these changes.
Therefore, the solution to the problem of malocclusion should be aimed at the entire complex of pathological changes: restoration of the anatomically correct position of the tongue, development of the correct stereotype of swallowing, chewing, head position, posture.
Osteopathic treatment offers exactly this approach: restoration or formation of the correct relationship of anatomical structures
- Correction of weakened or excessively tense muscles of the face, neck, floor of the mouth and the tongue itself, this will lead to the restoration of the correct position of the tongue in the oral cavity and uniform participation of the corresponding muscle chains in the processes of chewing and swallowing.
- The effect on the bone structures that form the cavities of the nose and mouth leads to the restoration of the physiological volumes of these cavities and helps improve nasal breathing, chewing, swallowing and speech.
- Motor innervation of the tongue, swallowing and chewing is provided by the hypoglossal nerve, which exits the cranial cavity through the canal of the hypoglossal nerve, where in some cases it may be compressed. Until a certain age, mobility is maintained in this zone and using osteopathic methods it is possible to restore the physiological correspondence of these anatomical structures.
Diagnostic measures
When undergoing a routine ultrasound examination during the third trimester of pregnancy, the doctor may detect congenital macroglossia. It is determined after comparison with the norms of each age at a given stage of fetal development. To make an accurate diagnosis, a repeat test is scheduled.
After the birth of the child, an examination awaits from many specialists - an infectious disease specialist, geneticist, otolaryngologist, endocrinologist. An instrumental examination is carried out, and a biochemical study of the blood fluid is prescribed. Based on the results of all tests and diagnostic methods, a diagnosis is made and therapy is prescribed.
Treatment methods
- If a protruding or sunken fontanelle indicates the course of a pathological process, treatment of the infant should be carried out in a hospital setting.
- If the baby is dehydrated, infusion therapy is prescribed.
- If the change in the fontanel is caused by an infection, then antibiotics, antiviral and anti-inflammatory drugs are used, and symptomatic treatment is prescribed.
- To relieve intracranial pressure, the child is given diuretics.
- In case of poisoning, enterosorbents are prescribed - drugs that cleanse the body of toxins.
In each individual case, the pediatric neurologist at our clinic decides on the issue of treating the baby, taking into account his individual characteristics.
When should you contact a neurologist?
Babies under one year of age are under constant supervision of a pediatrician. At each scheduled examination, a specialist must evaluate the condition of the fontanel. If the pediatrician sees a deviation from the norm, he will refer the child for a consultation with a neurologist. But there are situations when a child needs emergency medical care. You should immediately consult a doctor if the retraction or protrusion of the fontanel is accompanied by the following signs:
- rapid rise in temperature to 40C;
- uncontrollable vomiting;
- convulsions;
- loss of consciousness;
- drowsiness and lethargy;
- refusal to eat;
- dry skin;
- appearance of the “marble skin” effect.
Attentive parents will always notice the changed state of the fontanel. But only a certified doctor can determine the cause of the problem. In Kaliningrad, you can consult a pediatric neurologist at the Edkarik clinic. A competent specialist will competently assess the baby’s condition and prescribe adequate therapy.
Why does the fontanel swell
Swelling in the crown area means that intracranial pressure has increased. Regardless of the child’s behavior, this condition of the fontanel should alert parents, since it can develop against the background of the following pathologies:
- encephalitis;
- meningitis;
- hydrocephalus;
- cerebral malaria;
- tick-borne borreliosis;
- traumatic brain injury;
- poisoning;
- polio;
- leukemia;
- heart failure;
- a brain tumor.
The fontanel protrudes in small children with anemia and metabolic disorders. This symptom may indicate vitamin A deficiency and hemorrhage. A short-term pulsation of the large fontanel is observed in children under one year of age with prolonged crying and coughing.
But, regardless of the reason that caused changes in this area, parents should definitely show their baby to a pediatric neurologist. The Kaliningrad Edkarik clinic employs the best specialists who can quickly identify the cause of a pulsating or sunken fontanel.