The patient can remove removable dentures on implants without the help of a doctor. They consist of an acrylic base reinforced with wire (not always) and crowns made of medical plastic. Orthopedic structures are attached to implants using a beam method, using spherical, equatorial abutments, and telescopic crowns. Removable prosthetics on implants are preferable to traditional removable ones: the products are smaller, more comfortable to wear, securely fixed in the mouth, do not require frequent relining, and last twice as long. But in comparison with fixed and conditionally removable dentures on implants, they have a shorter service life.
- When used:
missing from 2 teeth - Type of anesthesia:
local - Procedure time:
60 minutes - Treatment period:
from 2 to 14 days - Healing period:
7-10 days - Age restrictions:
from 18 years old
Removable prosthetics on implants are preferable to traditional removable ones: the products are smaller, more comfortable to wear, securely fixed in the mouth, do not require frequent relining, and last twice as long. But in comparison with fixed and conditionally removable dentures on implants, they have a shorter service life.
Prosthesis design
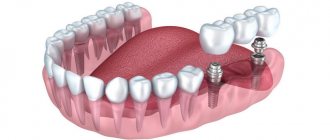
Removable dentures on implants are orthopedic structures that the patient can remove independently for care, with some effort. The structures consist of:
- acrylic or nylon base - imitation of natural gums;
- base made of metal wire - to impart rigidity to the frame (reinforcement is not always carried out and only in complete structures
); - crowns - often made of plastic, less often of ceramics, metal-ceramics, zirconium;
- fixation elements - one part of the fasteners is built into the prosthesis, the second - on the tops of artificial roots.
Removable dentures on implants are inexpensive designs. Prosthetics are carried out in order to save money and as a temporary option if it is not possible to install conditionally removable or fixed structures.
What are they made of?
Most often, the frame of such prostheses is made of plastic, nylon or acrylic, but today the implant must meet the highest quality standards, look believable, and also be made of hypoallergenic materials.
Metal ceramics
Popular due to:
- affordable price;
- having simple maintainability;
- long-term fixation (with proper manufacturing and care, 10-15 years);
- high strength;
- good looking;
- absence of allergic reactions.
Dentists recommend installing a metal-ceramic prosthesis in the following cases:
- violation of the shape of the dentition;
- change of enamel color;
- allergic reaction to the composition of the product;
- the absence of one molar in the chewing zone (molars are the sixth, seventh and eighth teeth of the permanent row or the fourth and fifth teeth of the deciduous row on the left and right sides of the jaw);
- increased abrasion.
Metal-plastic
These dentures are made from a metal frame and plastic crowns. They have already lost their relevance. In dental centers, this type of prosthetics is only for testing, for a short time (3 years). Doctors recommend installing this if you are missing one or more teeth, increased sensitivity and abrasion of tooth enamel.
Advantages of metal-plastics:
- quick installation;
- The design practically does not injure the mucous membranes.
Flaws:
- It is difficult to match the color of plastic so that it is similar to the color of enamel;
- If used on an ongoing basis, periodontal disease and caries may develop;
- Short service life;
- Plastic elements can cause an allergic reaction.
Implant attachment options
Removable structures are fixed to implants using beam and push-button fastening.
Beam fixation
Beam fastening is used on classic implants. The implanted artificial roots are connected by a metal permanent beam, which unites them and serves as part of the fastening of the orthopedic structure. The base of the prosthesis has a second part of the fastening - a recess in the shape of a beam, into which silicone holders are installed in the projection of the implants. When putting on the prosthesis, both parts of the fastening meet, the structure is securely fixed.
Due to the beam, the chewing load is evenly distributed between all implants. The quality of fastening is higher in comparison with push-button ones, but it also costs more.
Push-button type
Push-button fixation is used on classic and mini-implants with spherical or equatorial abutments.
- Ball mount.
After classic implants are implanted, spherical abutments are screwed into them, which protrude above the mucosa. Mini-implant designs already have a built-in aba. In the base of the orthopedic design, in the projection of each installed implant with an abutment, there is a recess with a metal holder for a silicone matrix and the matrix itself - a rubber sealing ring. When the product is put on, the ball-shaped abutment passes through the ring and is securely fixed with it. The disadvantage of prosthetics on spherical abutments is their wear due to friction. The heads become flat, the sealing ring no longer holds them - the abutments have to be changed or mini-implants must be reinstalled. - Equator mount on abutments
(Locator system). The principle of fixation remains the same, the shape of the abutment and the type of interaction between the head and the silicone matrix change. Constructions on equatorial abutments are easier to remove and easier to care for.
The advantage of push-button fastening is its low price. The downside is the relative instability of the product and the uneven distribution of the load on the implants.
On telescopic crowns
The essence of the method is to make a double crown. One is called primary and covers the prepared supporting implant. The secondary crown is larger, it is built into the frame of the prosthesis and covers the primary crown. The result is a reliable fixation system in the form of two crowns, which can be separated without effort and, if desired, the product can be removed.
Fixation of removable dentures on mini-implants
Removable prosthetics are performed using classic or mini-implants. The first option is reliable, but more expensive.
Mini-implants are smaller in size, have a diameter of 1.8 to 2.4 mm - they are not able to withstand heavy loads and have a limited service life (the products are worn for up to three years).
Two methods of fixing a removable product on mini-implants are used: using spherical abutments and using the Locator system. Dentures are installed immediately after implantation of mini-roots. The beam type of fastening is not used.
Dental prosthetics with mini-implants are chosen by patients who are financially limited or have contraindications to fixation of classic titanium roots.
What problems can be solved by installing a beam prosthesis?
This orthopedic design is indicated for patients who have lost a large number of teeth in a row, or the entire dentition. If there are still teeth in the oral cavity that cannot be restored for objective reasons (severe destruction), we remove them, relieve the inflammatory process and install implants.
Contraindications to prosthetics using this method relate primarily to implantation. It is not suitable for patients who have the following problems:
- serious pathologies of the cardiovascular system;
- disorders of blood clotting and tissue regeneration;
- oncological diseases;
- autoimmune diseases.
As for the metal beam, it is made from alloys that do not cause allergies, do not oxidize, and do not emit toxic substances.
Complete removable lower jaw prosthesis
For lower jaw prosthetics, up to six artificial roots should ideally be used. But if the bone tissue allows, 2 to 4 implants (whether classic or mini-products) are permissible to fix a removable denture. This is due to the increased density and thickness of the lower jaw bone.
When implanted with titanium roots into high-quality jawbone, structures of any length and diameter have excellent primary stability.
The use of traditional implants is always preferable, but in the case of the lower jaw, the installation of mini-implants is justified for the patient.
How templates for implantation are made
To obtain a template with maximum positioning accuracy, 3D modeling technology is used. And production is entrusted to specialized dental laboratories. First of all, the patient is examined on a computed tomograph, then impressions of both jaws are taken. Then the casts are scanned (digitized) and combined with the data obtained during tomography. Based on the information received, a 3D model of the template is created, on which the exact location of future implants is determined using computer modeling. The final stage of creating an implantation stencil is the implementation of the virtual model into a real object using CADCAM computer technology.
Dentures for completely edentulous upper jaw
Up to 8 implants are implanted into the jawbone from above, since the bone here is loose and subject to atrophy (compared to the lower jaw). In some cases, removable prosthetics of the upper jaw are organized on 4-6 implants, if the density and size of the bone allows.
If there is a significant deficiency of bone tissue, there is a risk of injury to the maxillary sinuses, then a sinus lift is performed first or mini-implants are used.
Mini-sized artificial roots are not the best option for fixing removable dentures on the upper jaw. Titanium roots will not stick to loose fabric. If mini-products are implanted, the Locator fixing mechanism is used.
How to avoid bone grafting?
There are proven methods that allow you to reliably restore teeth on one or both jaws without additional operations to build bone tissue.
First of all, it’s worth talking about the positions in which implants are installed. Humans have a total of 32 teeth, 16 teeth on each jaw. The 2 outer teeth are wisdom teeth; they do not bear a functional load, therefore they are not restored during prosthetics. Of the remaining 14 teeth (7 on each side), the most problematic in terms of restoration are the sixth and seventh teeth (counting from the center). They are located close to the maxillary sinus in the upper jaw and to the nerve in the lower jaw. It is precisely to restore the sixth and seventh teeth that lengthy osteoplastic operations are necessary.
According to the recommendations of the international association of implantologists ITI - International Team for Implantology , in the case of complete absence of teeth, it is necessary to restore the dentition up to the sixth tooth inclusive (12 teeth on each jaw). This method completely restores both the function of the jaw and the aesthetics of the smile. At the same time, additional risks associated with the close location of anatomically important formations (maxillary sinuses and nerve) are avoided.
In this case, the implants are installed in the anterior part of the jaw, and the outer ones in the area of the fifth teeth (the so-called Frankfurt University protocol ). Subsequently, a one-piece fixed prosthesis is installed on them. Combining all implants into a single structure compensates for lateral chewing loads and ensures full functioning of the entire jaw with only 6 implants in the lower jaw and 6-8 in the upper jaw.
Another problem is a deficiency of bone tissue thickness ( thin bone ). To avoid bone grafting in this case, it is possible to use thin implants. However, not all systems guarantee that their thin implants can withstand the load of full jaw prosthetics. Such guarantees are provided by German implants Ankylos , and the Straumann has developed a special alloy of titanium and zirconium, which allows thin implants to function without building up bone tissue, it is called Straumann Roxolid .
And lastly, if there is a deficiency of bone tissue both in height and width, a possible solution is to install short and thin implants, but in larger quantities. Instead of 6 standard ones - 8 short ones. The total length of the implants in this case will be equal.
Stages of prosthetics
- Preparation.
The doctor determines the size of the bone and excludes contraindications - the patient is given an X-ray, CT or OPTG, and sent for tests. Sanitation of the oral cavity is carried out. In case of bone deficiency, if there are no areas of the jaw with sufficient tissue volume, osteoplasty is performed before classical implantation. - Installation of implants.
In the classical protocol, implantation is organized using the patchwork method, and after implantation of titanium roots, sutures are applied. Mini-products are screwed into the bone through small holes (without cutting tissue or sutures). - Prosthetics.
With the classic protocol, the dentures are securely fixed in the mouth after the artificial roots have completely engrafted (after 3-6 months). During this time, the patient wears conventional removable dentures. When choosing mini-models, the prostheses are fixed 2-3 days after surgery.
Important!
When installing any orthopedic structures supported by their own teeth or implants, the patient should not feel discomfort. An incorrectly selected prosthesis leads to disruption of the chewing muscles and jaw joint. In our Center, all prosthetic work is carried out taking into account the patient’s bite characteristics; in difficult situations, consultations and treatment are provided by a gnathologist.
How does the procedure work?
Attachment of microprostheses occurs as follows:
- metal paws in the teeth, localizing the defect. Form grooves where the prosthesis is attached;
- special cement. The micromodule is fixed on adjacent incisors using a solution that is polymized under the influence of ultraviolet radiation and chemically;
- micro locks. The matrices are attached to adjacent teeth or crowns standing on them.
The last two methods make structures invisible to humans and others.
Advantages
In comparison with conventional removable dentures, designs supported by implants differ favorably in terms of reliability of fixation, service life and other characteristics.
| Classic dentures | Dentures on implants | |
| Reliability of fixation | not securely fixed, may fall out | securely fixed (fastening parts are located inside the prosthesis) |
| Duration of addiction | rub the mucous membrane, create discomfort | quick adaptation due to small size |
| Bone atrophy | do not stop the process of bone atrophy | pauses when the chewing load is evenly distributed (beam fastening) |
| Effect on gums | dentures put pressure on the gums, which lose their shape and atrophy | practically no pressure on the gums |
| Relocation | require regular relining due to sagging fabric | relocation is needed in the first months |
| Food restrictions | Do not eat hard, sticky foods | no restrictions |
| Difficulty of care | after every meal | periodically to remove plaque and clean the abutments |
| Life time | up to 5 years | up to 10 years with proper use |
Alternatives to removable implant prosthetics
An alternative to removable prosthetics on implants is the installation of a long-lasting prosthesis within the framework of a one-stage protocol using one of the methods:
- Basal implantation.
Implants are implanted into deep layers of bone that are not subject to atrophy (bone grafting can be eliminated). In case of complete edentia, the prosthesis restores the entire dentition; 14 artificial crowns are fixed on the jaw, since the “right” number of titanium roots are installed. A titanium arch runs inside the prosthesis, which unites and stabilizes the implants. Fixation can be screw (conditionally removable prosthetics on multi-unit implants) or cement (fixed prosthetics on basal or compression implants). - Everything is 4.
The prosthesis is supported by two implants in the frontal area of the jaw and 2 implants on the sides. The orthopedic design includes only 10 artificial teeth, since the lateral implants are fixed in the “fives” area, which limits the length of the prosthesis. Fixation can be screw or cement. We have modernized the protocol - if the situation allows, we add 1 more implant on each of the chewing sides, which allows us to install the “correct” prosthesis of 14 crowns.
Basal implantation Possibility to install implants without bone grafting with prosthetics in a few days
All-on-4 Fixed dental prosthetics on four implants with complete edentia
Removable dentures Recommended if there are absolute contraindications to implantation or if there is a limited budget
All-on-4
The All-on-4 technique (all-on-four) was developed by Nobel Biocare. It involves the installation of 4 implants on one jaw with simultaneous loading with a fixed prosthesis on a screw fixation. The 2 outermost implants are placed at an angle of up to 45 degrees, which allows you to bypass anatomically difficult places: the maxillary sinuses in the upper jaw and the nerve exit site in the lower jaw.
Initially, the All-on-4 technique was positioned as minimally invasive, without bone grafting. However, for successful functioning it is necessary to install sufficiently long implants, because 4 implants must bear the load of the entire dentition. Unfortunately, not all patients have the required alveolar ridge height. Installing shorter implants may result in one of the implants not taking root due to increased load. And then everything-on-four will turn into nothing-on-three. This is why patients are offered “all-on-4 modifications”, for example All-on-6 (all-on-six implants), because Installing an additional 2 implants significantly reduces the risks.
3-6 months after implantation using the All-on-4 method, gaps appear between the prosthesis and the gum, because This is why gum remodeling occurs after implantation. It is necessary to either reline the existing prosthesis or replace it with a permanent one - metal-ceramic or zirconium.