The most common dental diseases that a child can develop are caries and pulpitis. However, there are more serious pathologies, and parents need to be aware of them.
One of these diseases is edentia, which is characterized by the absence of teeth. This disease affects both primary and permanent teeth and can develop at any age. There are four main types of edentia:
- depending on the number of missing teeth - complete or partial. The first type is uncommon, diagnosed in only 3-5% of people;
- in accordance with the causes of the disease - primary (congenital) or secondary (arising during life).
Edentia of twos can also occur - the absence of paired front teeth located in the central part of the jaw.
Lack of teeth in humans: what is it and what does it mean?
What is jaw edentia? If in some species of animals the dentition is renewed continuously or at least repeatedly (for example, in Indian elephants), then people have only two sets of teeth - milk and molars. Unfortunately, they can be lost during life, and with some types of anomalies and diseases, a person initially lacks one, several or even all tooth germs. Adentia is a situation where there is a lack of teeth on one or both jaws. In this case, the absence of eights is not taken into account, since they are a rudiment and may not appear in principle. Experts highlight the absence of primary and molar teeth. In the latter case, the loss is irreparable. Therefore, most often they talk about edentulous molars, taking into account the fact that all the most negative consequences of this disease are especially pronounced in adulthood.
What does missing teeth affect?
- Chewing dysfunction.
- Problems with the digestive system.
- Deterioration of aesthetics. The most noticeable consequence of edentia. A diagnosis of “missing teeth” is often a death sentence for a beautiful smile.
- Bone tissue atrophy. Without the load that the teeth bear, the bone tissue begins to dissolve. When there is a lack of teeth, over time the face seems to shrink in the lower part and those same senile sunken cheeks appear. This is a consequence of bone atrophy.
- Curvature of teeth. In the absence of teeth, the bite is disrupted and the dentition shifts. It also distorts a person's facial features.
- Problems with diction.
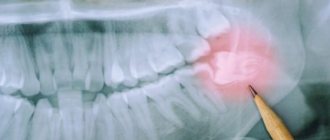
Unlike many dental diseases, signs of missing molars (as well as milk teeth) are very obvious. Diagnosis of edentia is usually carried out visually. However, to assess the condition of the bone tissue and the entire dentofacial apparatus as a whole, an x-ray examination is necessary. Now that it has become clear what jaw edentia is, it is necessary to talk about the causes and types of the disease.
Diagnosis of the disease
Adentia is a disease that is treated by specialists from different areas of dentistry:
- therapy;
- orthopedics;
- surgery;
- orthodontics;
- periodontics;
- implantology.
First, traditionally, anamnesis is collected, the necessary examination and examination are carried out. Based on the data obtained, the specialist compares the condition of the teeth and the patient’s age. If there is a hole in which a tooth has not grown, a targeted X-ray examination is performed; if there are many holes, a panoramic photograph of the dentition from the inside (or orthopantomography) is taken. Sometimes a specialist prescribes a CT scan of the joints to clarify the diagnosis. A detailed study reveals the presence or absence of tooth germs, hidden roots, tumors, and exostoses in the gums. In addition, the doctor has the opportunity to examine the tissues of the alveolar processes and detect symptoms of inflammatory processes.
Next, a plan for the treatment of edentulism is developed, in parallel with this, impressions are taken, and special artificial models of the patient’s jaw are produced for diagnostic research.
Causes of edentia
The problem of missing teeth sooner or later arises in almost every person. However, the causes of edentia can be very different. It all depends on whether it is primary (lack of tooth germs as such) or secondary (loss of already formed teeth).
| Primary causes of edentulism | Causes of secondary adentia |
|
|
VI. GENERAL ISSUES
Partial absence of teeth (partial secondary edentia) is one of the most common diseases: according to the World Health Organization, it affects up to 75% of the population in various regions of the globe [13].
In our country, in the general structure of medical care for patients in dental treatment institutions, this disease makes up from 40 to 75% and occurs in all age groups of patients [9, 13, 19].
Partial absence of teeth (partial secondary adentia) directly affects the patient’s quality of life. Partial absence of teeth (partial secondary adentia) causes disruption, up to complete loss, of a vital function of the body - chewing food, which affects the processes of digestion and the intake of necessary nutrients into the body, and is also often the cause of the development of diseases of the gastrointestinal tract of an inflammatory nature .
No less serious are the consequences of partial absence of teeth (partial secondary edentia) for the social status of patients: disorders of articulation and diction affect the patient’s communication abilities; these disorders, along with changes in appearance due to loss of teeth and developing atrophy of the masticatory muscles, can cause changes in the psycho-emotional state, up to mental disorders.
Partial absence of teeth (partial secondary adentia) is also one of the reasons for the development of specific complications in the maxillofacial area, such as the Popov-Godon phenomenon, dysfunction of the temporomandibular joints and the corresponding pain syndrome.
Untimely restoration of the integrity of the dentition in the case of their partial absence (partial secondary adentia) causes the development of such functional disorders as overload of the periodontium of the remaining teeth, the development of pathological abrasion, and disturbances in the biomechanics of the dentoalveolar system.
Untimely and/or poor-quality treatment of partial absence of teeth (partial secondary adentia) leads to the development of diseases of the dental system such as periodontal disease, and in the long term - to complete loss of teeth - complete secondary adentia of both jaws.
The concept of “tooth loss due to an accident, tooth extraction or localized periodontitis” (K08.1 according to ICD-C - International Classification of Dental Diseases based on ICD-10) and terms such as “partial secondary edentia” and “partial absence of teeth” ( in contrast to edentia - a disorder of the development and eruption of teeth - K 00.0), are essentially synonymous and are applied both to each of the jaws and to both jaws. A synonym for the terms “partial absence of teeth” and “partial secondary edentia” is also the concept of a dentition defect, meaning the absence of one or more teeth.
Partial absence of teeth (partial secondary adentia) should be distinguished from primary adentia, in which a defect in the dentition has developed due to the absence or death of the rudiments of permanent teeth. Partial absence of teeth (partial secondary adentia) is a consequence of caries and its complications, tooth extraction and/or loss due to an accident (trauma), periodontal disease, etc.
Caries in our country is one of the most common diseases. Its prevalence in adults aged 35 years and older is 98-99%. The rates of caries complications are also high: the percentage of extractions in the age group over 35-44 years is 5.5, and in the next age group - 17.29% [33]. In the structure of dental care in terms of visits, patients with pulpitis, which, as a rule, is a consequence of untreated caries, make up 28-30% [32].
The incidence of periodontal disease in the age group 35–44 years is 86% [31].
These diseases, if untimely and poorly treated, can lead to spontaneous loss of teeth due to pathological processes in periodontal tissues of an inflammatory and/or dystrophic nature, to the removal of teeth that cannot be treated and/or their roots due to deep caries, pulpitis and periodontitis.
Untimely orthopedic treatment of partial secondary adentia, in turn, causes the development of complications in the maxillofacial area and the temporomandibular joint, and also aggravates the process of tooth loss.
The main sign of partial absence of teeth (partial secondary adentia) is the absence in the dentition of one to fifteen teeth on one of the jaws [8, 35].
The clinical picture is characterized by the absence of one or more teeth in the presence of one or more natural teeth or their roots. Manifestations of partial absence of teeth (partial secondary adentia) depend on the topography of the defects and the number of missing teeth and are varied.
A feature of this pathology is the absence of pain syndrome in patients. In the absence of one or two, and sometimes several teeth, patients often do not feel discomfort and do not consult a doctor.
The partial absence of even one tooth in any functionally oriented group of teeth can lead to the development of the Popov-Hodon phenomenon, direct or reflected traumatic nodes, resulting in inflammation in the gingival margin, destruction of bone tissue and the development of pathological pockets, primarily in the area of the teeth , limiting the defect.
In the absence of one or more frontal teeth in the upper jaw, the clinical picture is characterized by the symptom of “retraction” of the upper lip. With a significant absence of lateral teeth on the soft tissues of the cheeks and lips.
In the absence of even one frontal tooth in the upper and/or lower jaw, diction may be impaired.
Partial absence of teeth in both jaws without preservation of antagonizing pairs of teeth in each functionally oriented group of teeth leads to a decrease in the height of the lower part of the face, often to the development of angular cheilitis (“jams”), pathology of the temporomandibular joint, changes in facial configuration, expressed nasolabial and chin folds, drooping corners of the mouth.
The partial absence of chewing teeth causes dysfunction of chewing; patients complain of poor chewing of food. Sometimes significant partial adentia is accompanied by habitual subluxation or dislocation of the temporomandibular joint.
After the loss or removal of teeth, atrophy of the periodontal ligaments occurs in the corresponding areas of the jaws; with the loss of more than two teeth, atrophy of the alveolar processes themselves gradually develops, progressing over time.
Partial absence of teeth (partial secondary edentia) is an irreversible process. Restoring the integrity of the dentition is possible only by orthopedic treatment methods using fixed and/or removable denture structures.
CLASSIFICATION OF PARTIAL ABSENCE OF TEETH (PARTIAL SECONDARY EDENTIA)
In clinical practice, partial absence of teeth (partial secondary adentia) of the upper jaw and lower jaw is not distinguished. The classification principles are the same for both jaws. The Kennedy classification of partial secondary adentia (dentition defects) has become most widespread and practically used [8, 14, 17].
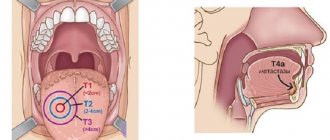
This classification distinguishes four classes: 1. Bilateral distally unlimited defect (end defect). 2. Unilateral distally unlimited defect (end defect). 3. Unilateral distally limited defect (included defect). 4.Lack of front teeth (defect in the frontal region) (included defect).
Each class has a number of subclasses. In the clinical application of the Kennedy classification, the doctor rarely encounters “pure” classes; variants of subclasses and/or a combination of defects of various classes and subclasses are much more often observed.
Another well-known classification of dentition defects is the classification of E.I. Gavrilova [8]. It distinguishes four groups of defects: 1. End one-sided and two-sided. 2. Included (lateral - one-sided, two-sided and front). 3. Combined. 4. Jaws with single teeth preserved.
Close to this classification is the Wild’s classification of defects [17, 54], which distinguishes the following main categories (classes) of partial secondary edentia: 1. Unilateral or bilateral terminal defect of the dentition. 2. One or more included defects. 3. Combination of terminal (terminal) and included (included) defects of the dentition.
In recent years, due to the importance of assessing the functional state of the dentition in partial secondary edentia, modifications according to Wild are increasingly used [17, 54].
When determining patient models, taking into account the functional state of the dentition and the possibility of restoring lost functions, which depends on the topography and the number of remaining teeth, it is more convenient to take as a basis the principle laid down in the classifications of E.I. Gavrilova and Wilda.
GENERAL APPROACHES TO DIAGNOSIS OF PARTIAL ABSENCE OF TEETH (PARTIAL SECONDARY EDENTIA)
Diagnosis of partial absence of teeth (partial secondary adentia) is made through a clinical examination, history taking and clinical examination. Diagnostics is aimed at eliminating factors that prevent the immediate start of prosthetics. Such factors may include the presence of:
- unsanitized teeth; — not removed roots under the mucous membrane; - exostoses; — tumor-like diseases; - inflammatory processes; - diseases and lesions of the oral mucosa.
When diagnosing, it is necessary to take into account the results of clinical and X-ray examinations of existing teeth, especially those planned for support, including their periodontal status, as well as the general and functional state of the dental system.
GENERAL APPROACHES TO TREATMENT OF PARTIAL ABSENCE OF TEETH (PARTIAL SECONDARY EDENTIA)
Basic principles of orthopedic treatment of partial secondary adentia:
1. When planning orthopedic treatment, the priority should be to preserve the remaining teeth.
2. Each tooth planned to support a prosthesis must be assessed from the perspective of the condition of hard tissues, pulp, periapical tissues, and periodontium. Depending on the results of this assessment, the support is determined as reliable, questionable or unsatisfactory. First of all, reliable teeth should be used for supports. The preservation of a tooth largely depends on its strategic importance as a support for the prosthesis, as well as on the ratio of labor intensity and cost of treatment measures necessary to preserve it and achieve results.
3. You cannot begin prosthetics without preparatory measures, if necessary.
4. Not every dental defect requires prosthetics. Prosthetics up to the complete set of dentition is not mandatory. The individual characteristics of the patient’s dental system play a decisive role.
5. Orthopedic structures should provide opportunities for optimal oral hygiene.
6. When making fixed bridges, structures of short length are preferred. Long structures that connect several functionally oriented groups of teeth into a single block should be avoided. Expanding the scope of prosthetics is justified only in conditions where this solution is the only opportunity to ensure optimal individual functioning of the dentofacial system.
7. Poor oral hygiene of the patient is a relative contraindication to fixed prosthetics.
8. The worse the patient follows medical recommendations and cooperates with the doctor, the simpler the orthopedic design should be [51].
The goal of treating patients with partial secondary adentia includes simultaneous solution of several problems:
— restoration of sufficient functional capacity of the dental system;
— prevention of the development of pathological processes and complications; — improving the quality of life of patients;
— prevention or elimination of negative psycho-emotional consequences associated with missing teeth.
Denture fabrication is not indicated if the existing denture is still functional or if its function can be restored (eg, repair, relining).
The manufacture of a prosthesis includes: examination, planning, preparation for prosthetics and all activities for the manufacture and fixation of the prosthesis, including the elimination of deficiencies and control. This also includes instructing and teaching the patient how to care for the denture and the oral cavity.
The orthopedic dentist must determine the features of prosthetics depending on the anatomical (taking into account the topography of defects in the dentition), physiological, pathological and hygienic state of the patient’s dental system.
When choosing between equally effective types of prostheses, the doctor should be guided by cost-effectiveness indicators. In cases where it is impossible to immediately begin and complete treatment as planned, the use of temporary prostheses, including removable or fixed immediate prostheses, is indicated. You can use only those materials, instruments, equipment, systems (for example, implantation), means of prevention and treatment that are approved for use by the Ministry of Health of Russia, clinically tested, the safety of which has been proven and confirmed by clinical experience. If there is a confirmed allergic reaction of oral tissues to the prosthetic material, tests should be carried out and the material that has proven to be tolerable should be selected.
When planning and conducting orthopedic treatment, it is necessary to take into account the health status, somatic status, and chronic diseases of the patient.
The most important stage of treatment is preparing the dental system for prosthetics.
Prosthetics should be carried out after the following measures:
— complete sanitation of the oral cavity should be carried out (pay attention to teeth with increased sensitivity);
— the feasibility of preserving teeth affected by caries and other diseases (x-ray and electroodontometric control), including filled ones, teeth with periodontal lesions, etc., should be checked when planning them as supporting ones;
— pulpless teeth must have roots sealed to the apex (x-ray control);
— the necessary treatment must be carried out for diseases of the periodontium and oral mucosa;
— if pathological processes in the teeth and jaw bones are suspected, it is necessary to conduct an X-ray examination;
- teeth and roots that cannot be preserved must be removed.
If a pathological process is detected on an x-ray, it should be eliminated before the fabrication of a permanent orthopedic structure. Any treatment aimed at eliminating oral diseases that prevent permanent dentures must be completed in full.
If it is impossible to completely eliminate pathological processes, primarily in the periapical tissues, prosthetics should take into account the possibility of subsequent surgical intervention. In such cases, radiological monitoring is necessary, no later than after 9 months [38].
Making a prosthesis for the jaw with partial secondary edentia includes: preparation of teeth, casts (impressions) from both jaws, production of diagnostic and working models, determination of the central relationship of the jaws, checking the design of the prosthesis, application, fitting, fitting, installation, fixation, remote control and corrections .
In the treatment of partial absence of teeth (partial secondary edentia), fixed bridges, cantilever fixed dentures, single crowns on teeth, partial removable plate and clasp dentures are used.
Bridges are usually indicated if:
- up to 4 incisors are missing, but chewing function is provided by natural teeth or existing bridges;
- in the area of lateral teeth on one side of the jaw no more than 3 teeth are missing and the dentition can be restored using a bridge with supports on both sides;
— the bridge will serve to fix the removable denture [51]. Thus, bridges are made with support on natural teeth on both sides (with the exception of cantilever ones). Bridges are not indicated:
- with insufficient ability of the periodontium to withstand loads and such general somatic diseases that adversely affect periodontal tissue;
- if an x-ray of the supporting tooth indicates a pathological process that cannot be stopped.
When replacing missing molars, the body of the bridge should be made with a wide wash (about 1 mm), not adjacent to the mucosa. In other areas of the jaws, the body of the bridge should not be adjacent to the mucous membrane (the tip of the dental probe should pass freely under the body of the bridge). It should be noted that the concept of a “tangential” intermediate part of a bridge prosthesis refers to a visual impression; in fact, a distance between the body of the prosthesis and the mucosa must be ensured, sufficient for free rinsing.
When using solid-cast metal-ceramic and metal-plastic bridges and crowns, a “garland” is always made from the oral side. Crowns with veneers and facets in bridges on the upper jaw are made only up to the 5th tooth inclusive, on the lower jaw - up to the 4th inclusive. The lining of the chewing surfaces of the lateral teeth is not shown in principle.
Crowns are indicated: - to preserve the tooth, if this cannot be achieved by other methods for a long time; - to protect the tooth from damage by the prosthesis; - for supporting the prosthesis; — to change the relationship of the jaws during prosthetics [51].
Artificial stamped and solid crowns for partial secondary edentia can be used to cover abutment teeth in the manufacture of removable partial laminar dentures and clasp dentures.
In the manufacture of artificial solid-cast crowns, four types of preparation are used, each of which has its own advantages and disadvantages, as well as recommended indications (Table 1).
Table 1
Clinical features of various forms of preparation of tooth stumps for crowns
| Preparation form | Advantages | Flaws | The appropriate type of prosthesis |
| Tangential (no shoulder) | Maximum preservation of hard tooth tissues, ease of implementation, smaller gap between the edge of the crown and the stump of the tooth in case of inaccuracy in the preparation form or errors during cementation | Lack of a clear preparation boundary, risk of excessive grinding of hard tissues, greater risk of trauma to the gingival margin | Solid crowns (without veneer), metal-ceramic and metal-plastic crowns with oral and vestibular garland |
| With a semicircular ledge | Clear preparation margin good distribution of impression, modeling and fixation materials relatively gentle method for hard tissues | The relative difficulty of solving the problem of prosthesis retention with a short clinical crown is the risk of complications (gingival recession) with an excessively convex veneer in the area of the gingival margin | Solid metal-plastic and metal-ceramic crowns |
| Preparation with a rectangular circular shoulder | Clear preparation margin Possibility to achieve optimal aesthetics due to sufficient space Low risk of excessive grinding in the cervical area | Large loss of hard tissues, danger of pulp damage, large cemented gap due to inaccurate preparation form or errors during cementation | Porcelain (jacket) crowns and half-crowns, metal-ceramic crowns with fired shoulder mass |
| Preparation with a shoulder-bevel at an angle of 135° | Clear preparation boundary, low risk of excessive grinding in the cervical area, smaller gap between the crown edge and the tooth stump in case of inaccurate preparation shape or cementing errors | Difficulty in performing, loss of hard tissue | Metal-ceramic and metal-plastic crowns, especially for front teeth |
In the case of partial absence of teeth and the impossibility of making a fixed bridge structure, as a rule, one-piece clasp dentures should be made. In this case, it is necessary to take into account the condition of periodontal tissues and the principles of hygiene.
As teeth are lost and the length of the toothless portion of the alveolar process (dentition defect) increases, the indications for the use of removable laminar dentures expand.
In the case of partial absence of teeth and the impossibility of redistributing the load on the periodontium of the supporting teeth, as a rule, partial removable lamellar dentures made of plastic without complex support-retaining elements are indicated.
The use of combined (combined) dentures is indicated if, using the necessary connecting elements and a sufficient number of preserved supporting teeth, it is possible to achieve functionally more favorable fixation and stabilization than using a clasp denture with clasp fixation or a partial removable laminar denture.
Connecting elements such as rod (beam) systems, telescopic crowns and attachments can only be used if the load is evenly distributed on the remaining abutment teeth.
In the absence of strict specific indications for prosthetics using dental implants, this type of treatment can only be used at the insistence of the patient on the basis of an appropriate agreement.
Primary and secondary edentulous teeth
Experts distinguish several types and subtypes of adentia. For greater convenience, below are tables showing the types of the disease, combined by certain characteristics.
Primary adentia
Caused by hereditary factors and diseases at the stage of fetal formation. With primary adentia, there is an absence of tooth germs.
Varies:
- partial primary adentia - the absence of one or more rudiments (for example, primary adentia of two incisors);
- complete primary adentia – absence of all tooth buds. It is extremely rare;
- true adentia – absence of tooth buds (without their destruction by diseases and infections);
- false edentia, when different teeth merge into one.
Secondary adentia
Secondary adentia occurs as a result of illness and injury during life.
Classification of edentulism by the number of missing teeth
| Number of missing teeth | Classes | general description |
| Partial edentia (ICD K00.00) | Partial primary adentia. Partial secondary adentia. | With partial edentia, from one to 5 teeth or their rudiments are missing on one jaw. Most often, three teeth are missing. |
| Multiple edentia | Multiple primary adentia. Multiple secondary adentia. | Many experts combine the concepts of partial and multiple edentulism. Criteria:
And so on up to 15 units on one jaw. |
| Complete edentia (ICD K00.01) | Complete primary adentia. Complete secondary edentia. | Complete absence of teeth or missing teeth |
Classification of missing teeth according to the location of the disease
| By localization | Description |
| Missing upper teeth | The absence of teeth in the upper jaw can be either partial or complete, as well as single. |
| Missing lower teeth | A general designation for a disease indicating the absence of teeth in the lower jaw. |
| Lack of chewing teeth | May be referred to as missing lateral teeth. Lack or complete edentulism in the chewing region. In particular, we are talking about the absence of small molars (premolars) and molars. |
| Missing front teeth | Edentia of incisors or canines in the frontal zone. |
In addition to the classification described above, the type of teeth itself is also taken into account. Based on this, the absence of molars and edentulous primary teeth (not associated with the normal timing of their replacement) are distinguished.
Differential diagnosis and treatment
To determine the pathology, the doctor should perform a full visual and instrumental examination of the oral cavity, and also find out:
- the reason and time period for retrieving units;
- previous illnesses;
- whether prosthetics have been previously performed.
During a consultative examination, the following is determined:
- asymmetry of facial features;
- pronounced folds on the chin and in the area of the nasolabial triangle;
- decreased height of the lower third of the face;
- seizures in the corners of the mouth;
- lip connection;
- wideness and pain in opening the mouth;
- mutual position of the jaws;
- TMJ crunch;
- level of thinning of the alveolar processes.
Palpation of soft tissues, mucosa and RG-TMJ is performed. Based on all the data, the doctor chooses the most appropriate treatment tactics (prosthetics, orthodontics).
Treatment of adentia
As has already become clear, the absence of teeth affects both functionality and aesthetics, as well as the overall quality of a person’s life. Treatment of adentia depends on the type, the presence of indications and contraindications for a particular prosthetic technique, as well as the financial capabilities of the patient.
Types of prosthetics in the absence of a large number of teeth and a single defect
| Type of edentia | Prosthetic options |
| Partial | Fixed bridge prosthesis, removable plate prosthesis |
| Plural | If there are a large number of missing teeth, a removable plate or clasp denture with hooks, clasps or attachments is used |
| Completely edentulous jaw | Plate dentures that completely imitate one of the jaws. Edentia of the lower jaw is complicated by the fact that the tongue and cheeks can displace the prosthesis, so prosthetics of the lower jaw in the absence of all teeth is carried out if there is no alternative. The same can be said about edentulism of the upper jaw, because A schematic denture with complete absence of teeth often falls out and can cause discomfort when worn due to the bulky base. |
Note: prostheses in the absence of classical type front teeth (bridges and circuits) are significantly inferior in terms of aesthetics to implant-based structures, therefore traditional prosthetics in the absence of teeth in the aesthetic zone are highly not recommended.
Implantation for edentia
| Type of edentia | Implantation options |
| Partial | Single implantation or fixed bridge prosthesis on implants. |
| Plural | Single implantation or fixed bridge prosthesis on implants. |
| Completely edentulous jaw | Dental implantation for completely edentulous patients usually follows certain protocols (“All on 4”, “All on 6”); however, if funds and positive indications are available, it is possible to install the maximum number of implants. |
Complications
Adentia entails disturbances of an anatomical and aesthetic nature:
- in the place of missing units, the toothless bone structure of the jaw becomes thinner over time;
- the symmetry of the face and the connection of the lips are disturbed, facial folds on the chin and in the nasolabial area deepen, the corners of the mouth droop;
- non-anatomical development of the jaws. It is more pronounced when there are a large number of missing units;
- with a numerous shortage of units at the LF, it begins to protrude forward and form a deep bite, moving into the HF.
Anatomical underdevelopment of the jaw bones does not always occur, and in children and adults it manifests itself differently. However, with all types of anomalies, negative clinical manifestations occur.
Important characteristics of complete or numerous adentia are the formation of a pathological bite and disruption of the digestive system. The bolus of food is difficult to chew, and the person has to limit his or her food intake. This pathology reduces self-esteem and makes you feel uncomfortable.