Structure of the TMJ
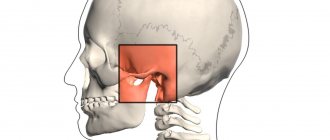
The temporomandibular joint (TMJ) is a paired joint projected in the area of the front of the ears, located at the place where the skull and lower jaw connect.
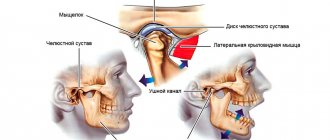
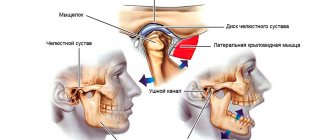
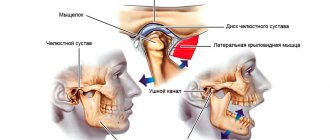
The anatomical structural elements of the joint are: the articular head; glenoid cavity; intra-articular disc dividing the joint cavity into the upper and lower floors, the articular capsule and the ligamentous apparatus.
TMJ pathologies include:
- muscular-articular dysfunction of the TMJ, as a result of internal disorders or joint disorders of the ligamentous-muscular apparatus
- arthrosis
- arthritis
- synovitis
- chondromatosis
- ankylosis
Musculo-articular dysfunction of the TMJ
Muscular-articular dysfunction of the TMJ can cause disturbances in the functioning of such muscle groups as mastication, facial expression, and cervical muscles; or cause intra-articular disturbances in the movement and position of the disc and (or) ligamentous apparatus.
Arthrosis
Degenerative changes in the TMJ are most often described by radiation diagnosticians and manifest themselves in the form of narrowing of the joint space on CT or MRI studies, which is a symptom of other TMJ diseases.
Arthritis
Inflammatory disease of the TMJ, the causes of which can be specific (tuberculosis, syphilis) or nonspecific infectious agents; and autoimmune and connective tissue diseases.
Ankylosis
Acquired or congenital disorder of TMJ mobility. It may be a consequence of hematogenous osteomyelitis as a result of umbilical sepsis, rheumatoid disease, trauma and is characterized by heterotopic bone formation and fusion of articular surfaces.
general information
Everything in the human body is interconnected. Changes in one organ area will cause a cascade of reactions throughout the body, including the musculoskeletal one.
Most medical practitioners do not look at the TMJ joint, but rather pay attention to the pain that occurs in different areas of the body due to TMJ dysfunction. Ascending postural causes of temporomandibular joint dysfunction are often associated with pelvic instability or instability of the sacroiliac joint. system - posture. Thus, postural instability of the body spreads upward, causing changes in the functioning of the temporomandibular joint. In addition, interactions at the dental level also affect the functioning of the TMJ.
When treating a patient's body for TMJ dysfunction and malocclusion, it is important to look at the entire system.
The pelvis is important for a balanced, stable position of the spine.
Inside the spinal column there is the dura mater, which also lines the cranial cavity from the inside, and is a single, inextensible, high-density structure. It is extremely important for the formation of the relationship between the skull and the spine. The dura mater has features in the places of attachment to bone structures, but we are especially interested in the sacrum and occipital bone, in the area of which the main fusion occurs. Thus, it is possible to trace the close relationship of the occipital bone and the sacrum, which normally should have synchronous movement. A dura mater stretched unnaturally as a result of scoliosis or pelvic pathology will directly lead to disruption of the functioning of both the occipital bone and the sacrum. Dysfunction in the pelvis quickly moves upward, causing pain in the neck, thoracic region, lower back, and finally affecting the function of the TMJ.
There is also an ascending type of dysfunction, in which problems in the lower levels of the body cause dysfunction in the upper parts. Now imagine that there is a leg injury or a spasm in the sacroiliac joint on one side. What will the body do? It will shift the main load to the healthy side (leg, or the side without pain and spasms).
The spine and the entire postural system of the body will adapt to the new center of gravity through body distortion. The distortion of the body will occur with the help of muscles that will contract or relax in a “chessboard” pattern, under the command of the central nervous system. Her commands will be aimed at maintaining body balance, because otherwise the person will simply fall on his side. This mechanism will also be reflected on the head, which will tilt in the opposite direction in order to maintain balance. Now let's look at the skull.
Intracranial pressure will automatically increase on the low side of the tilt and with a prolonged position of the head, the skull will tend to equalize this pressure. The central nervous system will once again give a command to the muscles of the anterolateral surface of the neck, the masticatory group. They will contract in such a way that the middle and anterior zones of the skull turn in the opposite direction, thereby balancing the intracranial pressure. Also, with the help of muscles, other mechanisms are implemented that maintain balance and postural balance of the body.
There are 3 powerful zones responsible for body balance:
1 - Eyes
2 - Vestibular apparatus
3 - Feet
If any of these systems fails, the load will be distributed among the others. Now imagine that when you tilt your head, caused by spasmed muscles of the back group (to maintain balance), information from the horizontal planes of the vestibular apparatus and eyes will become incorrect. In an attempt to align the signals, the brain will also give a command, and the neck muscles will contract, trying to rotate the middle and anterior zones of the skull closer to the horizon, i.e. align your eyes.
Treatment
Treatment for TMJ can range from conservative dental and medical treatments to complex surgical procedures. Depending on the diagnosis, treatment may include a short course of anti-inflammatory, painkillers and drugs aimed at muscle relaxation, special mouthguards/plates/splint therapy, consultation with medical specialists on psychological problems and stress.
If non-surgical treatment is unsuccessful or if there is obvious joint damage, surgery may be recommended. Surgery may involve arthroscopy and arthrolavage (a technique identical to orthopedic procedures used to examine and treat large joints such as the knee) or removing damaged tissue and replacing it with implants.
After diagnosing and making the correct diagnosis for problems with the temporomandibular joint, our specialists will provide the appropriate treatment necessary for a particular case.
TMJ dysfunction - symptoms and treatment
There is no single, universal method for treating TMJ dysfunctions. Full treatment may be hindered by pain that does not allow the necessary therapeutic measures to be carried out.
Conservative therapy allows you to relieve acute manifestations of pathology, ensures the weakening or complete disappearance of symptoms and restores the function of the lower jaw in full.
Physiotherapy is effective in reducing pain. To reduce pain, fluctuarization is used in the TMJ area. The essence of the procedure is the use of alternating, partially or fully rectified low-voltage electric current with a chaotically varying oscillation frequency. Fluctuarization helps reduce pain after 2-3 sessions. If the myogenic nature of the pain is caused by myositis (inflammatory damage to the skeletal muscles) due to contact involvement of the muscle in the inflammatory process, then treatment should first of all be aimed at eliminating the cause of the inflammation.
Amplipulse therapy (sinusoidal modulated current therapy) has shown effectiveness in the treatment of myofascial syndrome (a chronic condition in which pain points form in muscle tissue), reducing the tone of spastically contracted muscles.
Pain of joint origin is treated by prescribing phonophoresis with hydrocortisone, which allows to relieve pain in the acute period and reduce inflammation.
All types of treatment must be carried out under the control of electromyography to assess the effectiveness, equalize and normalize the electrical potentials of the muscles.
During complex treatment, the patient himself must perform myogymnastics after proper training in the technique. It includes passive and active exercises for the moving muscles of the lower jaw and neck muscles. Passive exercises are carried out without load; the patient needs to perform various movements of the lower jaw. Active exercises also include various movements of the lower jaw, but with a load (the patient’s arms counteract the movement being performed) [3]. Exercises should be done 3 times a day for 10-15 minutes.
To normalize bite and occlusal disorders, special orthopedic treatment methods are used - correction of occlusion and the use of orthopedic structures (splints, mouth guards, bite blocks, myostimulation, etc.).
Surgical treatment methods are used for serious morphological pathological changes in the joint. The main indication for surgical treatment is anterior displacement of the intraarticular disc.
Surgical treatment consists of focal chondroplasty of the disc or head of the lower jaw using autologous cartilage (usually nasal cartilage). It is also possible to reduce the disc and suturing the stretched intra-articular ligaments and joint capsule. These methods are aggressive for a complex articular system and they do not always give good results [11].
In the complex issue of treating TMJ dysfunction, over time, the most effective scheme has proven to be the use of medication, manual therapy, physiotherapy and orthopedic treatment aimed at restoring the dentition and normalizing the bite.
Anatomy of the TMJ
Home / Articles / Anatomy of the TMJ
The functioning of the TMJ (temporomandibular joint) determines the condition and health of the dental system, as well as the body as a whole. Due to its proper operation, the normal implementation of processes such as chewing, speaking, and movement of the lower jaw is ensured. Every day the TMJ performs thousands of movements, but the work of the joint is invisible, since it is hidden in the cheek and temple area. The balance of the TMJ normally allows a person to freely move the lower jaw, open and close the mouth, the imbalance does not appear immediately, but is also noticeable by the characteristic features that the orthodontist Farida Yusifovna Gasimova tells us about.
— Farida Yusifovna, how does the temporomandibular joint work?
— The structure of the joint is very complex, unlike other components of the internal structure of the body, its work does not in any way affect the functioning of the blood vessels, ear, nerves, although the joint is located directly next to it. This, one might say, is a perfect device that clearly and fully fulfills its role in the functioning of the body. Thanks to the paired design, uniform movement of both sides of the jaw is ensured simultaneously and equally. The anatomical structure of the TMJ includes the heads, fossae, capsules, ligaments of the articular tubercle, stylomandibular ligament and retroarticular disc. The active movement of the lower jaw relative to the upper is ensured by the structure of the head of the lower jaw, which has the shape of an ellipse, so the lower jaw easily moves forward and backward, right and left, up and down. The movable support is provided by the condylar processes at the end of which the head of the lower jaw is located. In children and adults, there are slight differences in the composition of the bone of the head, since with age new movements and functions are acquired, and the bone is overgrown with cartilage. Also, the size and shape of the head of the lower jaw is individual for each person since it is formed depending on the development and various factors of a person’s life; with age, changes occur in its structure. Next to the temporal bone and the zygomatic process and tubercle there is a mandibular fossa, which is separated from the auditory canal by a bone plate, and from the tympanic cavity by the posterior fornix. This structure allows you to avoid the development of pathological processes. The fossa is fenced off by the tympanic fissure, the zygomatic process, the sphenoid bone and the tubercle. The mandibular fossa is divided into extracapsular and intracapsular, and changes shape over the course of a person’s life. The articular tubercle becomes smaller in old age, this is associated with jaw deformation and loss of teeth; in newborn children it is absent altogether and is completely formed by the age of 7-8 years. Depending on the condition of the dentofacial system and teeth, the articular tubercle develops individually. The articular disc dentistry Millennium Anapa Mayakovsky is nourished through the fluid of the periarticular tissues and lymph; nerve endings do not approach it. The articular disc is located in the area of the tubercle and head. Depending on the type of jaw, the individual thickness and shape of the articular disc is formed. Movement of the disc and head is provided by ligaments woven into a dense capsule consisting of endothelial and fibrous connective tissue. Thanks to the work of the ligaments, the lower jaw moves up, down, sideways, forward and backward. Also, the ligaments restrain the stretching inside the TMJ and fix the joint.
— Farida Yusifovna, what specific function does the temporomandibular joint perform?
— The temporomandibular joint has many functions, the main one of which is to ensure the process of chewing, speech, pronunciation of sounds and movement of the lower jaw. Also, the temporomandibular joint is a unique human organ, consisting of two connected parts - right and left, which move equally and in parallel, have the same structure and structure. Together they are combined into a single complex system, with synchronous balanced movement. When synchrony is disrupted, TMJ dysfunction is diagnosed. The temporomandibular joint transmits impulses to the central nervous system, thereby ensuring chewing processes. The trigeminal nerve functionally connects the dentition on the lower and upper jaws and muscles; together this represents a complex biological system. The reflex activity of the TMJ ensures synchrony and parallelism of movements and the touching of teeth. If an imbalance occurs, it is necessary to carry out timely treatment, otherwise the person’s bite will be deformed and the teeth will be worn out.
— What does the term TMJ dysfunction mean?
— Disorders of the temporomandibular joint appear due to problems in the movement of the temporomandibular joint, which occurs simultaneously on both sides of the head. A violation is called uneven movement on the left and right sides when there is asymmetry. TMJ diseases can be very different, the most common are arthritis and arthrosis, ankylosis, synovitis, tendonitis, joint dislocation. Disturbances in the functioning of the TMJ cause pain and discomfort in the facial area; the causes may be mechanical injuries, malocclusion, damage to the jaw, poor-quality surgical intervention or dental treatment, infection, stress, genetic predisposition, anatomical abnormalities of the structure, excessive loads, pathologies of tooth abrasion. Dysfunction manifests itself initially weakly, many patients do not notice the symptoms until their brightness acquires colors in the form of closing of the jaw, crunching and clicking when moving the jaw, pain and itching, displacement of the jaw when opening the mouth, pain radiating to the ear, temple, swelling of the face, dizziness, tinnitus and other characteristic signs of TMJ dysfunction. The appearance of such symptoms should be a reason to contact Millennium Anapa Mayakovsky Dentistry.
Comprehensive hygiene for 2500 rubles! Air Flow 1000p for patients with braces!
A unique promotion for our regular patients! A set of hygienic procedures (removal of tartar and plaque using Air Flow and ultrasound , scaling, polishing, fluoridation) for regular patients once every 6 months for RUB 3,000!
Air Flow and polishing for only RUR 1,500 for patients with braces!
The temporomandibular joint (TMJ) (articulatio temporomandibularis) , formed by the head of the mandible and the mandibular fossa of the temporal bone (Fig. 1-24).
Rice. 1-24. Temporomandibular joint (TMJ) . A: 1 - zygomatic arch; 2 - zygomatic bone; 3 - coronoid process of the lower jaw; 4 - maxillary bone; 5 - second molar; 6 - lower jaw; 7 - third molar; 8 - masticatory tuberosity; 9 - branch of the lower jaw; 10 - stylomandibular ligament; 11 - condylar process of the lower jaw; 12 - anterior (outer) part of the lateral ligament of the temporomandibular joint; 13 - posterior (internal) part of the lateral ligament of the temporomandibular joint; 14 - mastoid process of the temporal bone; 15 - external auditory canal.
B: 1 - sphenoid sinus; 2 - lateral plate of the pterygoid process of the sphenoid bone; 3 - pterygospinous ligament; 4 - spine of the sphenoid bone; 5 - neck of the lower jaw; 6 - sphenomandibular ligament; 7 - styloid process of the temporal bone; 8 - condylar process of the lower jaw; 9 - stylomandibular ligament; 10 - opening of the lower jaw; 11 - wing-shaped hook; 12 - pterygoid tuberosity; 13 - angle of the lower jaw; 14 - mylohyoid line; 15 - molars; 16 - premolars; 17 — fangs; 18 - hard palate; 19 - medial plate of the pterygoid process; 20 - inferior nasal concha; 21 - sphenopalatine foramen; 22 - middle turbinate; 23 - superior nasal concha; 24 - frontal sinus
The head of the lower jaw is a roller-shaped thickening of an ellipsoidal shape, elongated in the transverse direction. The axes, extended along the length of the head, converge at the anterior edge of the foramen magnum, forming an obtuse angle. In front of the head, in the pterygoid fossa, the lateral pterygoid muscle is attached. The posterior surface of the head is slightly convex, triangular in shape, with the base facing upward. The articular surface of the mandibular fossa is 2-3 times larger than the head of the mandible. It has an elliptical shape. The fossa is divided into two parts: anterior - intracapsular and posterior - extracapsular. The incongruity between the head and fossa is leveled by the articular disc and the attachment of the joint capsule on the temporal bone. The intracapsular part of the articular fossa is limited in front by the slope of the articular tubercle, and in the back by the petrotympanic fissure. From the outside, the fossa is limited by the root of the zygomatic process, from the inside by the angular spine of the sphenoid bone. The shape of the mandibular fossa is different and depends on individual development factors, as well as the nature of dental occlusion. There are two extreme forms - deep and flat.
One of the characteristic features of TMJ is the presence of an articular tubercle, which is unique to humans. The articular tubercle, limiting the fossa in front, is a bony prominence of the zygomatic process. There are two extreme forms of the tubercle: a low and wide tubercle corresponds to a flat mandibular fossa, a high and narrow one corresponds to a deep fossa (Fig. 1-25).
Rice. 1-25. Shape of the articular tubercle : a - flat; b - medium-convex; v - cool
The articular disc (discus articularis) consists of fibrous cartilage tissue. It divides the joint cavity into two isolated slits - upper and lower. The disc has the shape of a biconcave lens, in which anterior and posterior sections are distinguished. Between the latter there is a thinner and narrower middle part of the disk. The anterior part of the disc is thicker than the posterior part. Its thickness depends on the shape of the articular fossa: the deeper and narrower the fossa, the thicker the disc, and, conversely, the flatter and wider the fossa, the thinner the disc (Fig. 1-26).
Rice. 1-26. Differences in the structure of the articular surfaces of the TMJ : a - ovoid shape of the condylar process and deep mandibular fossa; b — flat shape of the condylar process and the mandibular fossa: 1 — mandibular fossa, 2 — articular disc, 3 — condylar process; 4 — mandibular fossa (bottom view), 5 — isolated condylar process
Therefore, two extreme forms of the articular disc are distinguished: with one of them, the articular disc is flat and thin, with the other, narrow and thick. The purpose of the disc is to equalize the discrepancy between the articular fossa and the head and, due to its elasticity, to soften chewing impacts. The superior joint space is located between the glenoid fossa and the articular tubercle and the superior surface of the articular disc. The lower articular space is limited at the top by the concave surface of the disc, and at the bottom by the articular head of the mandible. The articulated surfaces in the lower joint gap fit one another more tightly, so it is narrower here than the upper one. The tendon fibers of the lateral pterygoid muscle are woven into the anteromedial edge of the articular disc, thanks to which it can move down the slope of the articular tubercle down and forward.
The articular capsule of the TMJ is extensive and flexible, allowing significant movements of the lower jaw. At the top, the capsule is attached anteriorly along the edge of the zygomatic arch, posteriorly along the fissura petrotympanica, medially along the spina angularis and sutura petrotympanica, then it turns outward and captures the articular tubercle in front. On the lower jaw, the capsule runs along the neck of the articular process, leaving the fovea pterygoidea outside the capsule. At the back, the capsule is thickened, and the extracapsular part of the mandibular fossa is filled with loose connective tissue, forming a maxillary cushion. The TMJ ligaments are divided into intracapsular and extracapsular . The intracapsular ligaments include the anterior and posterior discotemporal ligaments, running from the upper edge of the disc upward and forward and backward towards the root of the zygomatic arch; lateral and medial disconomandibular, located from the lower edge of the disc down to the attachment of the capsule at the neck of the lower jaw. Three ligaments are extracapsular. 1. The lateral ligament (ligamentum laterale) starts from the base of the zygomatic process and the zygomatic arch, goes down to the neck of the articular process. The ligament has the shape of a triangle, with the base facing the zygomatic arch, and consists of two parts: the posterior one, in which the fiber bundles go from above and forward, and the anterior one - the fiber bundles go from top to bottom and back. This ligament inhibits the lateral inward movements of the lower jaw. 2. The sphenomandibular ligament (ligamentum sphenomandibulare) originates from the angular spine of the sphenoid bone, extends downward, attaching to the lingula of the lower jaw. The ligament delays the lateral and vertical movements of the lower jaw.
3. The stylomandibular ligament (ligamentum stylomandibular) runs from the styloid process of the temporal bone down to the posterior edge of the ramus of the mandible. This ligament inhibits the forward movement of the lower jaw. The TMJ is a combined joint. Its articular surfaces are covered with fibrous cartilage. According to the nature of the movements, the joint is classified as block-shaped. The lowering and raising of the lower jaw is possible in the joint. With a slight lowering of the lower jaw, movement occurs around the frontal axis in the lower joint gap, while the head of the lower jaw produces rotational movements along the lower surface of the disc. The forward movement of the lower jaw occurs in the upper gap of the joint. In this case, the head together with the disc is one piece and slides forward and down the slope of the articular tubercle. Simultaneously with this movement, the head of the jaw makes rotational movements in the lower gap of the joint. Lateral movements of the lower jaw occur due to unilateral contraction of the lateral pterygoid muscle and the anterior bundles of the temporal muscle of the opposite side. The angle of deviation towards the lower jaw is 15-17°. The head of the jaw on the side of the contracting muscles makes its way down and forward onto the articular tubercle along with the disc, while turning inward. The movement occurs in the upper gap between the upper surface of the articular disc and the slope of the articular tubercle. In the joint of the opposite side, where the lower jaw has advanced, the head remains in the articular fossa, performing rotational movements around the vertical axis. In addition, the head shifts backward and inward. Movement occurs in the lower chamber of the joint between the lower surface of the disc and the articular head (Fig. 1-27).
Rice. 1-27. Sagittal section of the temporomandibular joint (TMJ)
In the joint cavity there is a biconcave Z-shaped curved cartilage disc. Since the lower jaw anatomically has two joints, it is classified as combined, complex, or biaxial. The movements in it are complex. The structure of the joint allows the lower jaw to perform rotational movements around the frontal axis - lower the jaw (open the mouth) to a distance of up to 5 cm between the front teeth in an adult. Further lowering leads to dislocation. If the mouth opens excessively, the condyle of the lower jaw can slip forward through the tubercle and be fixed in this position by muscle contraction. All this causes dislocation of the lower jaw, which can be on one or both sides. In this position, movements of the lower jaw are impossible, there is no speech, only inarticulate sounds are made. The dislocation must be reduced, and as quickly as possible, otherwise the stretched capsule creates conditions for repeated phenomena. But this must be done by a doctor, since inept reduction can be complicated by a fracture of the neck of the condylar process of the mandible. Since the joints are separated from each other, movements in them can be separate. This is facilitated by the wide capsule and ellipsoidal shape of the condyle of the jaw, i.e. presence of a vertical axis. More precisely, it is possible to move the jaw forward in one joint, but not to do this in the second joint, thus, in a non-adjustable joint, the condyle rotates around a vertical axis. The chin part of the jaw moves in a circle around the center. This displacement is limited by the joint of the opposite side and, above all, by the depth of its fossa of the temporal bone, the severity (height) of the articular tubercle and the strength of the articular ligaments. From the average position, the chin can move to the sides by no more than 15-17°, i.e. by 4.5% of the circumference. In addition to these movements, the jaw can move forward and backward simultaneously in both joints: this movement is called translational. Thus, the TMJ is the only joint that allows translational movements. Combinations of the described movements create the ability to chew, not only squeezing, but also crushing food by the shear type (move the jaw forward, sideways). The relief of the teeth also serves this purpose.
Materials used : Anatomy, physiology and biomechanics of the dentofacial system: Ed. L.L. Kolesnikova, S.D. Arutyunova, I.Yu. Lebedenko, V.P. Degtyareva. — M.: GEOTAR-Media, 2009
You might be interested in:
- Incisors (dentes incisivi). There are 8 incisors located in the middle of the dental arches, they are called the front teeth. There are upper and lower incisors, as well as medial...
">Structure of incisors
- Human teeth are an integral part of the masticatory-speech apparatus, which is a complex of interacting and interconnected organs...
">General structure of teeth
We recommend reading:
- General information about the structure of the human skull. The skeleton of the head is made up of paired and unpaired bones, which together are called the skull, cranium. ...
">Structure of the human skull
- Lower jaw The lower jaw (mandibula) is unpaired, horseshoe-shaped, the only movable bone of the skull. It consists of two symmetrical...
">Structure of the lower jaw
- Upper jaw The upper jaw, maxilla, paired, is located in the center of the face and connects with all its bones, as well as the ethmoid, frontal and…
">Structure of the upper jaw
The structure of the temporomandibular joint and bite problems
These problems, in the usual way for us, are associated with dental visits. However, there are a number of complaints that we are used to sharing with doctors of other specialties. These may be headaches in the back of the head and neck, dizziness, pain in the ear or ear (we are not talking about ENT diseases in this case), noise, clicking, crunching, increased tension or local, prolonged pain in the temples, a feeling of tension in the muscle areas of the neck, back of the head, temples, in the morning. But many of these problems are typical for patients with temporomandibular joint dysfunction. (Figure 1)
And it is very important to diagnose and prevent it in a timely manner, in the early stages of the development of pathology.
Let's try to figure out which patients may be at risk. To do this, it is necessary to obtain primary information about the structure of the temporomandibular joint.
The lower jaw (articular surface of the head) and the temporal bone (articular surface of the mandibular fossa) take part in the formation of the joint. The head of the lower jaw has an ellipsoidal shape. The mandibular fossa also has an ellipsoidal shape, but its articular surface is more than twice the size of the head of the mandible. The joint cavity is divided into two floors by the articular disc. The shape of the disk is compared to a biconcave lens. With the help of intra-articular ligaments, the disc is fused along the periphery with the joint capsule, so normally the two levels of the joint are isolated from each other. The articular disc acts as a shock-absorbing system in the area of connection of the lower jaw with the temporal bone. (Figure 2).
On the other hand, the fixing link or limiter of movements of the lower jaw is the plane of closure of the dentition of the upper and lower jaws (occlusal plane). In the case of healthy dentition, with all teeth present and in the correct position, the temporomandibular joints are in a balanced state, the articular discs are in a position between the bony structures of the joint and cope with their shock-absorbing function without much strain. At the same time, all the muscles involved in chewing, speech production and facial activity are also in a balanced state, i.e. all elements of the system evenly distribute their functions among themselves.
Let us now try to analyze several examples of violations of the harmony of the functioning of the dental system and their possible consequences.
A very clear example is the absence of one or more teeth. In such a situation in the oral cavity, the chewing process is disrupted, the patient involuntarily begins to chew on the side where the integrity of the dentition is not compromised, i.e. one of the sides becomes a priority for chewing. If a dental defect is restored in a timely manner (within several months), then, as a rule, such an uneven load goes unnoticed by the entire system. But even in this situation, pathological functional changes occur, muscle strain on the side where chewing was carried out, and even slight mobility may occur in the area of the teeth that have taken on additional load. All these phenomena disappear with timely restoration of the missing tooth(s). If the problem is left unresolved, these changes will progress to an irreversible phase; the muscle fibers remain in a hypertonic state and cause clenching of the teeth even in a calm state. Tooth mobility in congested areas may increase. Another option for the reaction of teeth to increased stress may be the abrasion of their hard tissues (enamel, then dentin).
Pathological changes also begin in the area of the TMJ (temporomandibular joint). With excessive, systematic compression in the area of one of the joints (with uneven chewing of food, for example), gradual abrasion of the articular disc occurs, which leads to the loss of its shock-absorbing ability, as well as to a change in its position and the position of the articular structures as a whole) (Fig. 3).
The trigger for the development of TMJ dysfunction can be many different factors, as well as their combination. The primary cause is often congenital characteristics of the bite, unnoticed and not eliminated in childhood and adolescence. In such situations, orthodontic treatment not carried out in a timely manner often causes combined violations of both the integrity of the dentition and joint dysfunction in adulthood.
But not always, when TMJ dysfunction occurs, as well as pain complaints in this area, the patient must have a serious pathology such as partial absence of teeth or malocclusion. Often some point irritating contact between the teeth of the upper and lower dentition is sufficient. Such contacts may appear due to the appearance of something new in the oral cavity, such as a filling or crown. Often, when restoring a damaged tooth with a new restoration, we are faced with the fact that over a short period of time it is necessary to adapt to the newly emerged sensations. In the case of simply becoming unaccustomed to contact with a damaged tooth, when it is restored, the patient will have a feeling of newness of the form, which is fleeting. This situation does not cause any disturbances or changes in the movements of the lower jaw during chewing. The muscles continue to work in harmony and harmony, as does the TMJ. If, when constructing the surface of a new tooth, some kind of tubercle or fissure (depression) appears, which, during chewing movements, causes changes in the movements of the lower jaw, over time this can cause serious complications. If this obstacle is not removed by the dental system on its own (a part of the restoration is chipped), then changes in the tension of the muscle fibers will occur. This tension will become uneven and sometimes too strong (hypertonicity). If this condition is not eliminated in a short time, then it becomes chronic and intensifies, and may already be an additional cause of increased tooth wear. Closed circle type mechanism. Subsequently, when the compensatory abilities of the articular disc are exhausted and it is no longer able to absorb and equalize the pressure and tension arising from uneven and asymmetrical movements in the area of the articular heads, pathological changes begin in the joint itself, causing dysfunction. TMJ dysfunctions are quite difficult to correct. To diagnose and understand them, additional research methods are required, which are individually selected by the doctor. An integrated approach in planning treatment for this category of patients is also very important. The participation of doctors not only from dental specialties is often necessary.
Specialists from our network of clinics will answer all your questions, offer to undergo the necessary diagnostic tests (teleradiography, orthopantomogram, computed tomography), draw up an individual treatment plan and tell you in detail about all its upcoming stages.
Material and methods
To study the morphological changes in the tissues of the TMJ, we analyzed the medical histories of 20 children with various pathologies of the antenatal period of development and diseases of early age, and also examined sectional material.
Morphological studies were carried out on the basis of the pathological department of the Regional Children's Clinical Hospital (head: E.S. Patlusova, candidate of medical sciences) in Perm. After opening, the organs were fixed in a 10% formalin solution for 24 hours, then they were processed using a Leica TP 1020 histoprocessor for 18 hours in alcohols of increasing strength and embedded in paraffin in a Histostar embedding station. Sections with a thickness of 3 microns were made from the finished paraffin blocks using a Microtom Hm 325 semi-automatic microtome with a given section thickness. Staining was carried out with hematoxylin and eosin for a review technique and according to Van Gieson to assess the degree of scleroplastic changes.
As an additional method, a morphometric study of organs was used. In this section, the thickness of the epithelial layer, the severity of perivascular edema, the thickness of the vascular walls and the width of the vascular lumens were assessed in order to assess the degree of emerging vascular disorders that could cause secondary changes in the organs of the oral cavity over time.
Morphometric study of the preparations was carried out using a binocular light microscope Axioskop 40 (´4, ×10, ×40) with a ×10 eyepiece and a computer image analysis system. It included: a light microscope, an Infinity 1 color video camera, an IBM compatible computer and software. The images (using the Infinity Analyze program) were digitized and transferred for subsequent storage to a computer hard drive. Computer image analysis was carried out using the Infinity Analyze program.