Scheme of forward and downward movements of the heads of the lower jaw
The TMJ provides a distal fixed position of the lower jaw in relation to the upper jaw and creates guiding planes for its movement forward, sideways and downward within the boundaries of movement. In the absence of contact between the teeth, the movements of the lower jaw are directed by the articulating surfaces of the joints and proprioceptive neuromuscular mechanisms. Stable vertical and distal interaction of the lower jaw with the upper jaw is ensured by the intertubercular contact of the antagonist teeth. The cusps of the teeth also form guide planes for the movement of the lower jaw forward and laterally within the contacts between the teeth. When the mandible moves and the teeth are in contact, the chewing surfaces of the teeth direct the movement and the joints play a passive role.
Vertical movements that characterize the opening of the mouth are carried out with active bilateral contraction of the muscles running from the lower jaw to the hyoid bone, as well as due to the gravity of the jaw itself.
Movement of the lower jaw when opening the mouth
There are three phases in mouth opening: slight, significant, maximum. The amplitude of the vertical movement of the lower jaw is 4-5 cm. When closing the mouth, the lifting of the lower jaw is carried out by simultaneous contraction of the muscles that lift the mandible. In this case, in the TMJ, the heads of the lower jaw rotate together with the disk around its own axis, then down and forward along the slope of the articular tubercles to the apexes when opening the mouth and in the reverse order when closing.
Sagittal movements of the lower jaw characterize the advancement of the lower jaw forward, i.e. a complex of movements in the sagittal plane within the boundaries of movement of the interincisal point.
The forward movement of the lower jaw is carried out by bilateral contraction of the lateral pterygoid muscles, partially the temporal and medial pterygoid muscles. The movement of the head of the mandible can be divided into two phases. In the first, the disc together with the head slides along the surface of the articular tubercle. In the second phase, the sliding of the head is accompanied by its articulated movement around its own transverse axis passing through the heads. The distance that the head of the mandible travels when it moves forward is called the sagittal articular path. It is on average 7-10 mm. The angle formed by the intersection of the line of the sagittal articular path with the occlusal plane is called the angle of the sagittal articular path. Depending on the severity of the articular tubercle and the tubercles of the lateral teeth, this angle varies, but on average (according to Gisi) it is 33°.
Biomechanics of the lower jaw during movement from central to anterior occlusion: O-O1 - sagittal articular path, M-M1 - sagittal path of the molar, P-P1 - sagittal incisal path; 1 - angle of the sagittal articular path, 2 - angle of the sagittal incisive path, 3 - separation (disocclusion between molars)
The sagittal occlusal curve (Spee curve) runs from the upper third of the distal slope of the lower canine to the distal buccal cusp of the last lower molar. When the lower jaw is advanced, due to the presence of a sagittal occlusal curve, multiple interdental contacts arise, ensuring harmonious occlusal relationships between the dentition. The sagittal occlusal curve compensates for the unevenness of the occlusal surfaces of the teeth and is therefore called the compensatory curve. In a simplified way, the mechanism of movement of the lower jaw is as follows: when moving forward, the head of the condylar process moves forward and down along the slope of the articular tubercle, while the teeth of the lower jaw also move forward and down. However, when encountering the complex relief of the occlusal surface of the upper teeth, they form continuous contact with them until the separation of the dentition occurs due to the height of the central incisors. It should be noted that during sagittal movement, the central lower incisors slide along the palatal surface of the upper ones, passing the sagittal incisal path. The angle formed by the vector of the incisal path and the occlusal plane. Depending on the elevation of the central incisor tubercles, this angle varies, but on average it is 40-50°. Thus, the harmonious interaction between the cusps of the chewing teeth, the incisive and articular tracts ensures the preservation of tooth contacts when the lower jaw is advanced. If the curvature of the sagittal compensatory occlusal curve is not taken into account in the manufacture of removable and fixed dentures, overload of the articular discs occurs, which will inevitably lead to TMJ disease.
The relationship between the sagittal articular and sagittal incisive tracts
Transversal (lateral) movements of the lower jaw are carried out as a result of predominantly unilateral contraction of the lateral pterygoid muscle. When the lower jaw moves to the right, the left lateral pterygoid muscle contracts and vice versa. In this case, the head of the lower jaw on the working side (displacement side) rotates around a vertical axis. On the opposite balancing side (the side of the contracted muscle), the head of the mandible slides along with the disc along the articular surface of the tubercle downward, forward and somewhat inward, making a lateral articular path. The angle formed between the lines of the sagittal and transverse articular path is called the angle of the transversal articular path. In the literature it is known as the “ Bennett angle ” and is equal, on average, to 17°. Transversal movements are characterized by certain changes in the position of the teeth. The curves of the lateral movements of the anterior teeth at the interincisal point intersect at an obtuse angle. This angle is called the Gothic or transversal incisal path angle . It determines the span of the incisors during lateral movements of the lower jaw and is on average 100-110°.
Vertical movement of the lower jaw.
The initial position of the lower jaw when opening the mouth is the state when the lips are closed. In this case, there is a gap of 2-4 mm between the dentition of the lower jaw and the upper jaw. This state is called a state of physiological rest. The movement of the lower jaw in the vertical plane occurs when opening and closing the mouth, due to the active contraction of the muscles: - depressors (mylohyoid, geniohyoid, anterior belly of the digastric muscle) - levator (proper masticatory muscle, temporalis, medial pterygoid muscle). The amplitude of mouth opening is strictly individual. On average it is 4-5 cm.
Phases of lowering the lower jaw.
1. With a slight lowering of the lower jaw (quiet speech, drinking), the articular heads in the infero-posterior part of the joint rotate around a horizontal axis passing through their centers. 2. With a significant lowering of the lower jaw (loud speech, biting), the hinge rotation in the infero-posterior part of the joint is joined by sliding of the articular heads together with the discs forward along the circumference of the articular surface. The result is a combined movement of the articular heads, in which the point of contact of two convex articular surfaces moves. 3. With the maximum lowering of the lower jaw, the sliding of the heads is delayed at the apex by the tension of the articular capsules, articular ligaments and muscles, and one hinge movement continues in the joint. The trajectories of movement of the lower teeth are concentric curves with a common center in the head of the lower jaw. They, just like the axis of rotation of the head, can move in space.
Movements of the lower jaw, bite and occlusal contacts of teeth
Opening the mouth. The initial position of the lower jaw when opening the mouth is the state when the lips are closed. At the same time, there is a gap of 2-4 mm between the dentition of the lower and upper jaw. This state is called a state of physiological rest.
The lowering of the lower jaw is carried out under the weight of the bone itself and bilateral contraction of muscles: the jaw - the hyoid muscle, the chin - the hyoid muscle, the anterior belly of the digastric muscle. There are 3 phases in the lowering of the lower jaw - slight, significant and maximum lowering. This corresponds to 3 types of movement of the articular heads.
A slight lowering of the lower jaw (quiet speech, drinking) occurs when its head moves in relation to the disc in the “lower floor” of the temporomandibular joint. In this case, identical movements simultaneously occur in the right and left joints along axes running along the greatest length of the ellipsoidal head of the lower jaw, and the midpoint of the central lower incisors describes an arc about 20 mm long.
With a significant lowering of the lower jaw (loud speech, biting) and hinge rotation in the “lower floor” of the joint, the articular heads, together with the discs, slide forward along the circumference of the articular surface, i.e. movement also occurs in the “upper floor” of the joint.
With the maximum lowering of the lower jaw, the sliding of the heads is delayed at the top of the articular tubercle by the tension of the articular capsules, articular ligaments and muscles. In this case, the midpoint of the lower incisors describes an arc up to 50 mm long.
Further excessive opening of the mouth can also occur with a slight hinge movement of the articular heads, but this is highly undesirable, since there is a danger of stretching of the ligamentous apparatus of the temporomandibular joint, dislocation of the head and disc.
Closing the mouth. Raising the lower jaw is carried out by contracting the muscles that lift the lower jaw (masseter, temporal, medial pterygoid) and the movements occur in the reverse order. The articular heads are displaced back and upward to the base of the slopes of the articular tubercles. The closing of the mouth is completed due to the hinge movements of the articular heads until occlusal contacts appear.
Movement of the lower jaw forward. After reaching the initial contact of the chewing teeth (centric relation), the articular heads move forward and upward - into central occlusion. At the same time, they move 1-2 mm along the midsagittal plane, without lateral displacements, with simultaneous bilateral contact of the slopes of the cusps of the lateral teeth.
The advancement of the lower jaw forward with the teeth closed from the central occlusion to the anterior one is carried out due to the contraction of the external pterygoid muscles on both sides. This movement is guided by the incisors. If the lower incisors in central occlusion are in contact with the palatal surfaces of the upper incisors, moving the lower jaw forward from this position causes disocclusion of the lateral teeth. The sliding continues until the cutting edges of the teeth of the lower jaw come into contact with the cutting edges of the teeth of the upper jaw. The path that the lower incisors take along the palatal surfaces of the upper incisors is the sagittal incisal path, and the angle between this path and the occlusal plane is the angle of the sagittal incisal path. During this movement, the articular heads move forward and down the slopes of the articular tubercles, making a sagittal articular path, and the angle between this path and the occlusal plane is called the angle of the sagittal articular path.
These angles and their individual determination for each patient are used to adjust the articulator - a device that simulates the movement of the lower jaw.
When moving the lower jaw forward between the dentition, contact is maintained at several points: between the incisors, between individual chewing teeth on the left and right sides. The cusps of the last molars of the lower jaw stand above the level of the cusps of other chewing cusps of the first and second molars of the upper jaw below the level of its other chewing teeth. These contacts in the literature are called the three-point Bonville contact or the Bonville triangle point. The sides of the triangle connect the centers of the right and left articular processes of the lower jaw and the incisal point and average 10 cm.
Lack of contact in the area of chewing teeth when biting, when there is occlusal contact on the incisors, can lead to overload of the latter, and with artificial dentition replacing a defect in the front teeth or a complete defect in the dentition (dentitions) - to the overturning of the dentures. This can cause overload of the joint, since the intra-articular disc, moved to the top of the articular tubercle, experiences increased pressure from the articular head, and the capsule and ligaments of the joint are stretched. If a three-point contact (according to Bonneville) is created on artificial dentition, then the pressure on the joint discs is reduced, the ligaments are stretched less, and the fixation of the prosthesis is better.
Lateral movements of the lower jaw
Rice. 10. Scheme of lateral movement of the lower jaw to the left in the horizontal plane (a), possible paths of movement of the head of the balancing side (b) and the “occlusal compass” (c):
A, B - initial position of the jaw;
A1, B1 - position of the jaw when shifted to the left;
B – B1 – Bennett movement;
B is Bennett's angle. The dotted line indicates “initial lateral movement”;
c - “occlusal compass” - a path that describes the supporting palatal cusp of the upper left first molar on the occlusal surface of the lower first molar shown in the figure;
E – forward movement;
G – movement to the left;
D – movement to the right.
During lateral movement of the mandible from the position of central occlusion, the articular head on the side of displacement (side of laterotrusion) rotates around its vertical axis in the corresponding glenoid fossa and makes a lateral movement, which is called Bennett's movement. This lateral movement of the working articular head averages 1 mm. The articular head on the opposite side (the mediotrusion side) moves downwards, forwards and inwards. The angle between this path of head movement and the sagittal plane is Bennett's angle (~ 17º). The greater the Bennett angle, the greater the amplitude of the lateral displacement of the articular head of the balancing side.
With a lateral displacement of the lower jaw, the lateral pterygoid muscle of the side opposite to the displacement of the lower jaw contracts, therefore, with a unilateral type of chewing, unilateral hyperactivity of the muscle can occur, which adversely affects the function and structure of the TMJ, the condition of the hard tissues of the teeth and periodontium.
When studying the structure of the dentition of the lower and upper jaws in the area of chewing teeth, the following was established:
a) the crowns of the chewing teeth of the lower jaw are inclined towards the tongue, resulting in an equal level of location of the buccal and lingual cusps;
b) the palatal cusps of the maxillary molars are located lower than the buccal ones.
As a result of different levels of arrangement of the cusps of the chewing teeth, lateral occlusal curves are formed that pass through the buccal and lingual cusps of both sides of the chewing teeth. Lateral occlusal curves ensure the preservation of occlusal contact in the area of the chewing teeth with a lateral shift of the lower jaw, which is equal to no more than half the width of the chewing teeth.
During lateral movements of the lower jaw, the occlusal relationship between the cusps of the antagonist teeth on the balancing and working sides is different. On the side of the contractile muscles, the antagonists meet with tubercles of the same name (working side), on the opposite side - with opposite tubercles (balancing side).
Literature:
- S. I. Abakarov, ed. E. S. Kalivradzhiyan “Fundamentals of dental prosthetics technology - a textbook for medical schools and colleges. Moscow, 2016. M.: “Geotar – Media”. pp. 130 – 146.
- I.V. Alabin, V.P. Mitrofanenko “Anatomy, physiology and biomechanics of the dental system” - M., “ANMI”, 1998, p. 73-93, 99-114, 178-181.
- Shcherbakov A.S., Gavrilov E.N., Zhulev E.N. “Orthopedic dentistry”, St. Petersburg: IKF “Foliant”, 1998, p. 44-51
Original work:
Movements of the lower jaw, bite and occlusal contacts of teeth
Sagittal movements of the lower jaw.
The forward movement of the lower jaw is carried out by bilateral contraction of the lateral pterygoid muscles. The movement of the head of the lower jaw is divided into 2 phases: 1- the disc together with the head slides along the surface of the articular tubercle; 2- the sliding of the head is accompanied by its articulated movement around its own transverse axis. The distance that the head of the mandible travels when it moves forward is called the sagittal articular path. This distance is on average 7-10 mm. The angle formed by the intersection of the line of the sagittal articular path with the occlusal plane is called the angle of the sagittal articular path. According to Gisi, it averages 33º. With an orthognathic bite, the protrusion of the lower jaw is accompanied by sliding of the lower incisors along the palatal surface of the upper ones. The path taken by the lower incisors when moving the lower jaw forward is called the sagittal incisal path. The angle formed by the intersection of the line of the sagittal incisal path with the occlusal plane is called the angle of the sagittal incisal path. On average, its value is 40-50°. Bonneville's three-point contact. When the lower jaw is advanced to the position of anterior occlusion, contact of the dentition is possible only at three points. Two of them are located on the distal cusps of the second and third molars, and one on the anterior teeth.
Lateral movements of the lower jaw (Gothic angle - 110° and Bennett angle - 17°)
These data are necessary for programming the articular mechanisms of devices that simulate the movements of the lower jaw. On the working side, the lateral teeth are positioned relative to each other by tubercles of the same name; on the balancing side, the teeth are in an open state.
The nature of the closure of chewing teeth in left lateral occlusion: a - balancing and b - working sides
It is known that the chewing teeth of the upper jaw have an axis inclined towards the buccal side, and the lower teeth - towards the lingual side. Thus, a transverse occlusal curve is formed, connecting the buccal and lingual tubercles of the chewing teeth of one side with the same tubercles of the other side. In the literature, the transversal occlusal curve is called the Wilson curve and has a radius of curvature of 95 mm. As noted above, during lateral movements of the mandible, the condylar process on the balancing side moves forward, down and inward, thereby changing the plane of inclination of the jaw. In this case, the antagonist teeth are in continuous contact, the opening of the dentition occurs only at the moment of contact of the fangs. This type of opening is called “canine guidance.” If, at the moment of opening the molars on the working side, the canines and premolars remain in contact, this type of opening is called “canine-premolar guidance.” When making fixed dentures, it is necessary to establish what type of opening is typical for a given patient. This can be done by focusing on the opposite side and the height of the fangs. If this cannot be done, it is necessary to make a prosthesis with canine-premolar guidance. In this way, overloading of periodontal tissues and articular discs can be avoided. Compliance with the radius of curvature of the transversal occlusal curve will help to avoid the occurrence of supercontacts in the chewing group of teeth during lateral movements of the lower jaw.
The central relationship of the jaws is the starting point of all movements of the lower jaw and is characterized by the highest position of the articular heads and the tubercular contact of the lateral teeth.
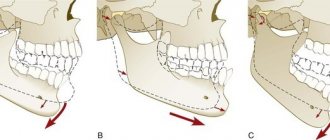
Mouth opening (A) from the position of centric relation (B) and central occlusion (C)
The mandible then slides to a more stable position where maximum fissure-tubercle contact is achieved. The sliding of teeth (within 1 mm) from the position of the centric relation to the central occlusion is directed forward and upward in the sagittal plane, it is otherwise called “sliding along the center.”
Movement of the lower jaw from centric relation (A) to centric occlusion (B)
When the teeth are closed in central occlusion, the palatal tubercles of the upper teeth come into contact with the central fossae or marginal projections of the lower molars and premolars of the same name. The buccal cusps of the lower teeth are in contact with the central fossae or marginal projections of the same upper molars and premolars. The buccal cusps of the lower teeth and the palatal cusps of the upper teeth are called “supporting” or “retaining”, the lingual cusps of the lower and buccal cusps of the upper teeth are called “guide” or “protective” (protect the tongue or cheek from biting).
Functional purpose of the tubercles: 1 - buccal tubercle of the upper molar - protective; 2 - palatal tubercle of the upper molar - supporting; 3 - buccal tubercle of the lower molar - protective; 4 - lingual tubercle of the lower molar - protective
When the teeth are closed in central occlusion, the palatal tubercles of the upper teeth come into contact with the central fossae or marginal projections of the lower molars and premolars of the same name. The buccal cusps of the lower teeth are in contact with the central fossae or marginal projections of the same upper molars and premolars. The buccal cusps of the lower teeth and the palatal cusps of the upper teeth are called “supporting” or “retaining”, the lingual cusps of the lower and buccal cusps of the upper teeth are called “guide” or “protective” (protect the tongue or cheek from biting).
Percentage ratio of supporting and guiding tubercles
During chewing movements, the lower jaw should slide freely along the occlusal surface of the teeth of the upper jaw, i.e. the tubercles should smoothly slide along the slopes of the antagonist teeth without disturbing the occlusal relationship. At the same time, they must be in close contact. On the occlusal surface of the first lower molars, the sagittal and transversal movements of the lower jaw are reflected by the arrangement of longitudinal and transverse fissures, which is called the “ occlusal compass ”. This landmark is very important when modeling the occlusal surface of teeth.