Bullae (false pulmonary cysts) are pathological air cavities in the lungs (from the English blebs - “bubbles”), which can arise due to mechanical damage to the parenchyma, a previous infectious-inflammatory or other disease. Excess air in these bag-like cavities, changes in the structure of the pulmonary matrix, and a reduction in the area of functional areas of the respiratory organ lead to persistent respiratory impairment, and the consequences of such pathological changes can be irreversible. The formation and enlargement of bullae in the lungs leads to a decrease in the gas exchange function of the lungs, and in the case of rupture of a large bulla, it can lead to a life-threatening condition - pneumothorax.
Interesting fact: air travel is dangerous for patients with large bullae in the lungs. The fact is that in flight at an altitude of 2.5 km from the ground, pathological cavities can increase in diameter by 30-40%, which means an episode of pneumothorax and rupture of the bulla may occur.
Bullae are most often diagnosed in people who smoke (usually men over 50 years of age with about 15 years of smoking experience) against the background of centrilobular pulmonary emphysema or COPD. Both of these diseases are in one way or another associated with damage (stretching) of the alveoli, disruption of the structure of the pulmonary parenchyma, and its aging. Sometimes these pathological changes are not associated with smoking, but are a consequence of metabolic disorders, an infectious-inflammatory process, an autoimmune disease, or are genetically determined.
The disease is difficult to treat. If the cause of the formation of bullae is established, their size is small, diagnostic measures are carried out on time and treatment is started, the pathological changes can be treated conservatively. In case of pneumothorax, bullae are removed surgically using endoscopic techniques.
Bullae require dynamic monitoring: CT scan, spirometry, consultation with a pulmonologist.
What does a bulla in the lung mean?
According to the definition given at the international medical CIBA symposium, a bulla should be considered an air cavity in the lung, the diameter of which exceeds 1 cm, while the alveolar wall thins to 1 mm or less.
In medicine, it is customary to distinguish between bullous emphysema and bullous disease. They are distinguished depending on the causes of occurrence, etiology, and also depending on the health consequences. Bullous emphysema is usually diagnosed in patients with signs of COPD (chronic obstructive pulmonary disease) against the background of bilateral emphysema of the panacinar or centrilobular type. With bullous disease, emphysema is not observed, and the cavity may be one or slightly larger. Bullous disease can occur with congenital Marfan syndrome. Bullous emphysema, in the absence of treatment and adequate actions to curb its growth (quitting smoking, working in hazardous industries, treating chronic bronchitis, etc.) over time can lead to respiratory or heart failure, lung collapse, severe coughing with blood, and physical intolerance. loads
Bullae are formed according to the principle of soap bubbles: first small ones appear, then they combine to form large bullae, and so on. With bullous emphysema, the lung tissue becomes like an old sponge - as it wears out, the pores become larger, and the material loses its elasticity and tears.
Large bullae (diameter can reach up to 10 cm) are formed when the alveolar septa are destroyed. Alveoli are vesicles that make up normal air lung tissue. Air storage, oxygen transportation, air exchange are carried out in the alveoli, and the process itself requires a structure of dosed air supply. Bullae, even very small ones, introduce an element of chaos and entropy into the work of the most important respiratory organ.
Rare complication of tonsillectomy: subcutaneous emphysema and pneumomediastinum
Chronic tonsillitis (CT) remains a very common problem today [1], especially considering that the main group of people suffering from CT are people of working age [2]. In different countries, according to various epidemiological studies, this disease affects from 4 to 15% of the population, and among all diseases of the pharynx, CT accounts for up to 35% [1, 3]. There is a trend towards an increase in the number of patients with chemotherapy, with the highest incidence observed in the age group of 16–20 years [3]. Tonsillectomy (TE) is a routine operation in the practice of an otolaryngologist. And although this operation is considered very safe, it is nevertheless associated with such possible complications as bleeding, infections, swelling of the tongue, injury to the glossopharyngeal nerve, and carotid artery. Very rare complications of TE are subcutaneous emphysema of the face and neck, pneumomediastinum and pneumothorax [4]. The literature describes just over 30 cases of the development of subcutaneous emphysema after TE [5]. Subcutaneous emphysema is a potentially life-threatening condition because it can progress to obstruct the passage of air in the upper respiratory tract or spread into the mediastinum, resulting in the development of pneumomediastinum or pneumothorax and depression of cardiorespiratory function [4]. According to the literature, the first described case of subcutaneous emphysema of the face and neck after TE dates back to 1933 [6]. Subcutaneous emphysema can develop either as a result of a pressure difference on both sides of the injured mucosa, or when gas is released by body tissues in a closed cavity [7]. Cervical emphysema and pneumomediastinum are usually caused by rupture of the tracheobronchial tree or esophagus. Subcutaneous emphysema is characterized by crepitus and can be easily detected by X-ray examination. The presence of pneumomediastinum can be assumed if symptoms such as shortness of breath, dysphagia, pain in the chest and back, cyanosis and Hammann's sign are observed - crepitus, synchronous with heart contractions and heard best when the patient turns on the left side [8]. A review of the literature demonstrated that indications for TE include frequent sore throats or a history of peritonsillar abscesses. The tonsil niche is bounded anteriorly by the palatoglossus muscle, laterally by the velopharyngeal muscle, and superiorly by the superior pharyngeal constrictor. In this regard, a possible reason for the development of subcutaneous emphysema after TE may be that the muscle layer, consisting of the superior pharyngeal constrictor, does not reach the upper pole of the tonsil; in this place, the pharyngeal wall consists of the mucous membrane and the pharyngeal aponeurosis (internal and external). With TE, the external aponeurosis may be damaged. Thus, during the operation, conditions are created for the penetration of air (during swallowing, coughing, vomiting) into the parapharyngeal space through the resulting hole. Emphysema spreads down the neck along the fiber of the vascular bundle [9]. There are reports in the literature that, deep in the tonsil niche, the superior pharyngeal constrictor creates a path through the soft tissues of the neck to the parapharyngeal, retropharyngeal and prevertebral spaces. If injury occurs at this location, air can enter the mediastinum through the deep cervical spaces and cause pneumomediastinum. In some rare cases, air that has entered from the mediastinum may then descend into the abdominal cavity through the diaphragmatic opening [10].
Clinical observation
The patient, 29 years old, was admitted to the ENT clinic with complaints of frequent sore throats, periodic pain in the throat, and snoring. From the anamnesis it was known that he had been ill for a long time, sore throats had been noted since childhood, 3–4 times a year. Courses of conservative treatment were carried out: washing the lacunae of the tonsils with antiseptic solutions, repeated courses of antibiotic therapy without significant effect. Over the past year, she suffered 3 sore throats, the last one in November 2015, was treated on an outpatient basis, and was given antibacterial therapy. Objectively upon admission: the general condition is satisfactory, the skin and visible mucous membranes are of normal color. The soft palate is symmetrical. The signs of Zach, Giese, Preobrazhensky are positive. The palatine tonsils are enlarged (grades II–III), dense, with caseous masses in the lacunae (Fig. 1). Regional lymph nodes are not enlarged and painless. The rest of the ENT organs are unremarkable.
TE was performed under combined endotracheal anesthesia, intubation was performed through the right half of the nose. The palatine tonsils were removed coldly; a pronounced scarring process was noted, especially on the left. Hemostasis - using a bipolar coagulator. Due to bleeding from the upper pole of the left tonsillar niche, the palatal arches were sutured. The volume of bleeding was up to 200 ml. There were no other peculiarities during the operation. The patient woke up in the operating room and was transferred to the ward. The patient complained of swelling, pain and a feeling of pressure in the left half of the face 5 hours after the operation. No coughing or difficulty breathing was noted; the act of swallowing was painful, but completely preserved. Physical examination revealed swelling and crepitus in the left half of the face, which extended into the submandibular, periorbital area on the same side, as well as into the upper neck (Fig. 2). No redness was noted in the swollen area. Examination of the pharynx did not reveal any pathological findings. Indirect laryngoscopy, anterior and posterior rhinoscopy revealed no pathological changes. Body temperature – 36.7°C. Clinical blood test: leukocytes – 13.9×109/l, erythrocytes – 4.12×1012/l, platelets – 271×109/l, hemoglobin – 128 g/l, hematocrit – 35.0%, neutrophils – 77 .0%; ASLO (antistreptolysin-O) – 359 IU/ml.
On the same day, the patient was transferred from the otolaryngology department to the intensive care unit for dynamic observation. According to ultrasound: air is detected in the soft tissues of the left cheek, the angle of the lower jaw on the left and the submandibular region at a depth of 7 mm from the surface of the skin. No fluid accumulations were detected. According to MSCT data of the pharynx, larynx and chest organs, subcutaneous emphysema was extended to the left buccal region, extending downwards into the left submandibular region, the side of the left orbit, the region of the parotid gland, neck and mediastinum. Air bubbles were detected in the posterior mediastinum along the esophagus and descending aorta (Fig. 3).
Therapy included meropenem 1 g 3 times a day IV drip for 5 days, famotidine 20 mg IV drip for gastroprotection, Ringer's solution, ketoprofen 2.0 IM for pain. During therapy, positive dynamics were noted: resolution of subcutaneous emphysema (Fig. 4); upon pharyngoscopy, the tonsillar niches were covered with fibrin plaque (Fig. 5). There was still slight pain when swallowing.
conclusions
Thus, taking into account the literature data and our observation, the treatment of patients with subcutaneous emphysema and pneumomediastinum includes regular assessment of respiratory function and the degree of emphysema. Any situation that increases pressure in the upper respiratory tract (coughing, vomiting, voluntary tension of the muscles of the throat and neck) or vigorous physical activity should be avoided. They recommend bed rest and sedation, restriction of food intake, as well as cough relief and stool regulation. Broad-spectrum antibiotics may be prescribed. In some cases, oxygen therapy is used for faster resolution of subcutaneous emphysema [5, 11]. We assume that the cause of subcutaneous emphysema was injury to the external aponeurosis of the pharynx due to a pronounced adhesive process. During the operation, noticeable adhesions were discovered between the tonsils and tonsil niches, which made the operation more time-consuming and traumatic. Postoperative factors that can contribute to the formation of emphysema are vomiting, coughing, constipation, when air can pass into the interfascial spaces through the damaged mucosa [12]. Other possible pathogenic mechanisms include rupture of the tracheobronchial tree at any location [13], resulting in the formation of pneumomediastinum, after which air spreads in a cephalic direction, secondary to subcutaneous emphysema of the neck. A defect in the tracheobronchial tree may be a consequence of an existing pathology: bullous alveoli, laryngocele. The defect can also occur due to injury to the laryngotracheal mucosa during intubation [14]. In our observation, subcutaneous emphysema of the neck, face and pneumomediastinum developed after planned TE. Subcutaneous emphysema and pneumomediastinum are rare complications of TE. The mechanism of their formation is not completely clear; air is believed to penetrate the tissue through the buccal-pharyngeal fascia [8]. If there is a history of paratonsillar abscesses and/or multiple sore throats, one should take into account the high probability of the possible presence of an adhesive process between the palatine tonsils and the tonsil bed and extremely carefully and carefully cut off the palatine tonsils from the surrounding tissues. This will likely reduce the risk of postoperative bleeding, as well as prevent the development of rare postoperative complications such as subcutaneous emphysema and pneumomediastinum. If examination reveals any macroscopically obvious mucosal injury in the niche area, the damaged mucosa can be sutured to prevent secondary bacterial complications and the development of subcutaneous emphysema or enlargement of already formed emphysema. In most cases, subcutaneous emphysema and pneumomediastinum resolve spontaneously. Not a single fatal outcome has been described in the literature; one patient with the same diagnosis had a tracheotomy [10], and two had a thoracotomy [6, 11]. However, it should be remembered that subcutaneous emphysema and pneumomediastinum can be potentially fatal complications.
Symptoms of bullous emphysema
A number of studies published in the open international database PubMed emphasize that factors such as:
- Smoking (15-20 packs);
- Systematic inhalation of toxic substances (unfavorable environment, work in hazardous industries, substance abuse, drug addiction);
- Low level of quality of life (poor and unhealthy diet, hypothermia, illness, lack of qualified medical care).
And only next to these factors in terms of prevalence are past infectious and inflammatory diseases of the respiratory tract, autoimmune diseases, metabolic disorders, and congenital characteristics of the body.
In the vast majority of cases, bullous emphysema is diagnosed in elderly or mature people, but bullae can also be found in young people.
Small bullae do not manifest themselves at all. In general, it is difficult for the patient to even suspect most diseases of the main respiratory organ - the lungs do not hurt, and when shortness of breath, coughing, and lack of air occur, the disease brings the patient to intensive care in a matter of hours.
Pathological symptoms may appear as the bullae enlarge and emphysema develops. Prevention of the disease is possible through regular screening - low-dose CT scan of the lungs. Examination in 3D mode and in high resolution will show even the slightest deviations from the norm.
To determine the (exact stage) of bullous emphysema, the method of spirometry is used - functional diagnosis of the lungs. As a rule, after spirometry, if the indicators are not normal, the pulmonologist sends the patient for a CT scan of the lungs.
Bullae in the lungs can be suspected if the following symptoms are present:
- Shortness of breath and breathing difficulties;
- Resistance to physical activity, fatigue;
- Hypotension, uncontrolled arrhythmias;
- Feeling of constant fatigue;
- Blue lips and fingertips;
- Painful pallor;
- Feeling of incomplete inspiration;
- Deformation of the chest (becomes barrel-shaped if there are large bullae).
Since the enlargement of bullae lasts quite a long time, the patient may not notice a deterioration in health, in particular, it becomes increasingly difficult to hold his breath due to a decrease in the vital capacity of the lungs, and hypoxia generally affects all internal organs - the person literally “fades.”
Subcutaneous emphysema after sinus lift
Subcutaneous emphysema is the result of air entering tissue spaces. This complication has long been described in the literature and, according to an analysis carried out by Heyman and Babayof in 1995, which involved systematizing the available data from 1960 to 1993, such a pathology does not develop often, but requires special attention to avoid the development of further associated complications. type of infection. The etiology of subcutaneous emphysema is associated with the use of high-speed burs and compressed air during restorative and endodontic procedures.
In the clinical case described below, subcutaneous emphysema developed several hours after sinus lift surgery, which makes this case somewhat special. Most often, postoperative emphysema is associated with certain actions of the patient after surgery (sneezing with the mouth closed, blowing the nose, playing wind instruments). The purpose of this article is to illustrate the possibility of developing orbital and periorbital emphysema after iatrogenic manipulation of the maxillary sinus and to inform the doctor about methods of treating such a complication.
Clinical case
A 52-year-old non-smoking patient sought help from the Department of Periodontology (University of Valencia, Valencia, Spain) for a preventive examination. During the analysis of the clinical situation, it was decided to restore the existing edentulous areas with the help of fixed dentures supported by dental implants (photo 1-2). The rehabilitation plan involved the installation of an implant 10 mm long and 4 mm wide distal to the second premolar of the maxilla on the left. Given the deficiency of bone tissue, it was previously necessary to perform an atraumatic sinus lift procedure in this area. According to cone beam computed tomography, the residual bone crest in the area of planned implantation was 5 mm. The patient had no contraindications to sinus lift or any other systemic diseases.
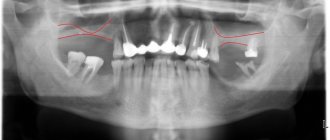
Photo 1. Periapical radiograph before treatment.
Photo 2. Orthopantomogram before treatment.
Surgical procedure
Two days before the intervention in the form of vertical augmentation of the bone tissue of the upper jaw in the area of the maxillary sinus, the patient was prescribed antibiotics (amoxicillin, 500 mg, 1 tablet every 8 hours for 7 days). 1 hour before surgery, the patient also took ibuprofen (600 mg, 1 tablet). Anesthesia of the intervention area was carried out using the infiltration method using articaine with an adrenaline concentration of 1: 100,000 (Ultracain, 40 mg; Normon; 3 carpules of 1.8 ml each). Next, a vertical incision was made mesial to the second premolar region, passing through the mucogingival line. After separation of the full-tissue flap, the molar was extracted and complete visualization of the intervention area was ensured. Access to the maxillary sinus was provided through a lateral window measuring 10 mm by 8 mm. The window was formed using a carbide bur and a piezosurgical attachment (Piezomed, W & H). 718-EN2, MC-1, and MC-2 hand separator instruments (Bontempi) were used to lift the Schneiderian membrane. A Valsalva maneuver was performed to check the integrity of the membrane. A membrane was then placed into the created space and volume was created using a bovine xenograft (Bio-Oss, 0.25–1.00 mm granules; Geistlich Biomaterials).
The total amount of xenograft used was 2.5 g. The lateral window was covered with a resorbable collagen membrane (Bio-Gide, Geistlich Biomaterials). Suturing was performed using Supramid sutures (5/0, round, non-absorbable; Steinerberg). Immediately after the manipulation, a control periapical radiograph (photo 3) and an orthopantomogram (photo 4) were taken. Postoperative recommendations included eating only soft and cold foods for the next few days, not smoking, and avoiding toothbrushing. Oral care was recommended by rinsing with 0.12% chlorhexidine solution (Perio-Aid, 0.2% chlorhexidine and 0.05% cetylpyridinium chloride; Dentaid) for 1 minute, 3 times daily for 10 days. If pain or swelling developed, the patient was allowed to take anti-inflammatory drugs.
Figure 3. Periapical radiograph after treatment.
Photo 4. Orthopantomogram after treatment.
Clinical monitoring and occurrence of orbital and periorbital emphysema
Onset and clinical signs
Three hours after surgery, the patient reported inflammation on the left side of his face, which developed immediately after three continuous sneezes (Figure 5). During the clinical examination, it was found that the patient did not have any pain symptoms, his vision was not impaired, although the resulting swelling somewhat limited the possibilities for the full opening of the eyelid. The muscular system of the eye was not damaged. During diagnostic orthopantomography, no changes were noted in the area of sinus lift. The patient was diagnosed with subcutaneous emphysema and prescribed amoxicillin 875 mg and clavulanic acid 125 mg, 1 tablet every day for 7 days.
Photo 5. Photo of a patient with subcutaneous emphysema.
Permission
By the third day, there was a visible decrease in emphysema and a decrease in signs of inflammation, which completely disappeared after 7 days. Emphysema resolved without any complications. The patient had no signs of pain or symptoms of infection.
Discussion
In the presented clinical case, subcutaneous emphysema appeared after severe sneezing in the patient several hours after the sinus lift procedure. The overall outcome was favorable, but the patient had to adhere to a specific medication regimen. Previously, many cases of subcutaneous emphysema as a complication, especially after dental procedures, had already been reported in the literature. The most common reason for its development is the use of tips operating under air pressure. Emphysema has also occurred in cases of crown preparation, primary and secondary endodontic procedures, and during the use of a dental laser.
It is extremely important to differentiate emphysema from hematoma or an allergic reaction. To do this, you need to collect anamnesis data, palpate and examine the area of edema. Emphysema is manifested by swelling without redness and crepitus of soft tissues. Several cases of emphysema of the orbital and periorbital region have already been described in the literature. Patients usually do not experience pain, but they may complain of some discomfort.
Air can penetrate into the parapharyngeal and retropharyngeal spaces, where its accumulation can compromise the patency of the airways and provoke the development of embolism and infection of soft tissues. Subcutaneous emphysema can also cause pneumothorax, optic nerve damage, and even death.
For a patient with subcutaneous emphysema, prophylactic antibiotics and close monitoring of the airway are recommended. The most commonly used antibiotics are amoxicillin and clavulanic acid.
Conclusion
This article describes a clinical case of the development of subcutaneous emphysema, which developed several hours after the sinus lift procedure as a result of the patient sneezing. This complication was treated with antibiotic therapy and close monitoring. The development of emphysema in no way compromised the outcome of subantral augmentation.
Authors: Luis Martorell Calatayud, Regino Zaragozí Alonso, Miguel Peñarrocha Diago, María Sevilla Heras
Bullae in the lungs on CT
Bullae in the lungs on CT are visualized as distinct, relatively darker, bubble-like areas of lung tissue, resembling holes or large pores of a sponge. The denser the tissue, the lighter it appears on CT scans—so, for example, bones are white, but airy lung tissue is a relatively uniform graphite gray color.
Using a CT scan of the lungs, a radiologist can accurately determine the diameter of the bullae, their number, and find out whether there are signs of emphysema, bronchiectasis or other diffuse pulmonary diseases.
How to treat bullae in the lungs
The patient needs to quit smoking and quit working in harmful production activities, otherwise all therapeutic measures will be meaningless. In uncomplicated cases and in the early stages of emphysema (or bullous disease), treatment is conservative and combined. Therapy is prescribed by a pulmonologist and may include:
- Medicines (diuretics, bronchodilators, hormonal drugs);
- A special course of exercise therapy and breathing exercises;
- Regular oxygen therapy using an oxygen concentrator.
- Regular diagnostic measures (CT of the lungs, spirometry, consultation with a pulmonologist).
The positive aspect is that complete and lifelong cessation of smoking in most patients stops the development of bullous emphysema, and the use of oxygen therapy in seriously ill patients can prolong life by 5-10 years.
Surgical treatment of bullae (endoscopic “suturing”) may be indicated for recurrent pneumothorax against the background of growing cavities. The patient undergoes bullectomy and pleurodesis operations. However, the absolute success of such treatment cannot be guaranteed.
Dental clinic ANO "Newstom Aesthetic", Irkutsk State Medical University
This work was published in the collection of scientific works “Problems and prospects of modern science” (2009, Volume 2, issue 1), edited by Prof., Doctor of Biological Sciences. Ilyinskikh N.N.
View the title page of the collection
Public awareness of legal aspects has changed significantly over the past 10 - 15 years. However, in contrast to the fairly large volume of legislation regarding the protection of patients' rights, the rights of doctors remain practically unprotected. Therefore, the only shield for a doctor can be high quality work, a high level of legal literacy and well-executed documentation. This determines the relevance of the problem of protecting the rights of doctors, especially in such a costly field in terms of material and emotional aspects as dentistry (Afanasyev V.V. et al., 2007). Increasingly, the Russian literature discusses the need to obtain informed consent from the patient before performing any intervention. Sergeev Yu.D., Erofeev S.V. (1998) believe that it is advisable to provide information about possible iatrogenic complications either in the information part of the contract for the provision of medical services, or in the approval sheet as an appendix to the medical history. Polushin Yu.S., Levshankov A.I. (1998) argue that the informed consent of the patient makes the risk of intervention an acceptable risk and protects the doctor from legal retribution. The problems of endodontic treatment complications have become especially acute in recent years - during the period of rapid development of instrumental technologies: high-speed turbine dental units, high-pressure hydropneumatic hygienic systems, and automatic irrigation devices. As a rule, the main reasons for the occurrence of difficult situations are: non-compliance with technological requirements during treatment, lack of practical skills, skills and theoretical knowledge, haste in carrying out manipulations. Complications that arise during endodontic treatment, according to the ICD-10 classification, are periostitis, osteomyelitis, phlegmon, lymphadenitis, cyst, chroniosepsis, fistula. However, this classification of complications does not include a nosological form that is quite common in clinical practice—airborne (surgical) emphysema of the soft tissues of the maxillofacial region. Surgical emphysema is the introduction of air or an air-liquid mixture under the skin (mucous membrane) and into the interfascial spaces of soft tissues, leading to a noticeable increase in tissue volume and tension of the skin with a change in their color. An acute toxic condition that accompanies surgical emphysema is manifested by severe pain and soft tissue swelling. Quite often, microorganisms enter the tissues along with the air, and then the situation can become more complicated. The entry of air (with microorganisms) into the blood vessels is called an air embolism. A pulmonary or cerebral embolism is a very serious and potentially fatal complication. We have not found a detailed description of the pathogenesis of liquid-air surgical emphysema in the maxillofacial area, provoking clinical situations, as well as treatment methods and outcomes of this problem in the literature. In the course of studying the specialized literature on dentistry, only one source found a mention that surgical emphysema develops when using an air turbine dental handpiece during endodontic treatment. To determine the awareness of doctors regarding this complication and their readiness to prevent its occurrence, as well as the tactics of managing patients with surgical emphysema, we conducted an anonymous survey of 86 dental therapists in the cities of Irkutsk, Angarsk, Shelekhov, Usolye-Sibirskoye, Ulan-Ude and Chita. The following questions were asked: 1. What complications of endodontic treatment have you encountered in practice? 2. Have you observed cases of pain and toxic damage to periradicular tissues from irrigants? 3. Under what circumstances did surgical emphysema of the soft tissues of the maxillofacial area occur? The study of the survey results made it possible to identify among all the complications two cases of air and air-liquid emphysema when using water-air guns during drying of root canals and cavities, three clinical situations when using high-pressure air-abrasive devices when carrying out hygienic measures, four cases of acute toxic complications with severe pain when removing irrigation solutions into periradicular tissues. After analyzing several clinical cases of the development of surgical emphysema at a dental appointment in clinics in the city of Irkutsk and the Irkutsk region, it was determined that complications, as a rule, arose due to non-compliance with the endodontic treatment protocol and gross violation of the technology for using irrigation solutions and high-pressure systems. Apparently, the individual anatomical and clinical characteristics of the patients were also not taken into account in each case of complication that arose. We have identified the main causes and conditions for the occurrence of complications. It has been determined that surgical emphysema, as a complication of endodontic treatment, occurs when using a turbine handpiece for root canal preparation; when drying root canals (especially maxillary molars) with compressed air; due to abundant irrigation under pressure of the root canal with antiseptic solutions, as well as when solutions of sodium hypochlorite and hydrogen peroxide enter the periradicular tissues through periodontal damage. Surgical emphysema can develop, in addition, when an air-water jet enters periodontal pockets on the vestibular surface of the lateral teeth of the upper jaw, as well as an air-abrasive mixture based on sodium bicarbonate - into periodontal pockets and defects of the buccal mucosa during hygienic procedures (air- flow). Based on studying the results of a survey of dental therapists and assessing the effectiveness of treatment of surgical emphysema of the maxillofacial area in the analyzed clinical cases, we formulated the following provisions. When using 3% hydrogen peroxide solution or 2.5-5.25% sodium hypochlorite solution as irrigants, it should be remembered that their use should be limited to the canal space. The release of these solutions outside the canal, especially under pressure, leads to severe toxic effects, tissue damage, as well as acute pain and swelling. These concerns prompt doctors to either abandon the use of these irrigants, replacing them with distilled water or saline, or significantly reduce the concentration of antiseptics used. However, this often results in a significant reduction in the effectiveness of the irrigant. According to the literature, for all of these problems, patients should be recommended to prescribe broad-spectrum antibiotics and non-steroidal anti-inflammatory drugs. According to the results of a survey of dentists, in cases of surgical emphysema, favorable outcomes were observed with the use of fourth-generation fluoroquinolones (Ciprofloxacin, 500 mg - 2 times a day), complex synthetic penicillins based on amoxicillin and clavulonic acid (Amoxiclav, 875 mg). According to dental surgeons who participated in the treatment of patients with surgical emphysema, as well as in the relief of toxic conditions due to the removal of sodium hypochlorite solution into the periradicular tissues, desensitizing therapy with the use of antihistamines and antiallergic drugs (Suprastin, Pipolfen, Tavegil) is effective, both orally (1 each tablet - 3 times a day), and parenterally (1-2 ampoules per day intramuscularly). In case of severe pain, injectable analgesics (Ketonal) are prescribed. If local hemosiderosis occurs, it is recommended to use a mixture of hydrocortisone with heparin ointment. Mandatory monitoring of body temperature and bed rest with limited motor function are recommended. If the doctor inadvertently inserts compressed air into the root canal, antibiotics should be prescribed immediately and the patient should be closely monitored. However, the basic principle of endodontics is to never use compressed air in root canals. We believe that timely use of antibacterial therapy and dynamic monitoring minimize the risk of irreversible changes in tissues. It is especially worth emphasizing the careful and attentive attitude towards the patient with this complication, since the patient needs to feel understanding and sympathy from the doctor. In addition, you should know that if a preliminary agreement has been reached about the possibility of harm to health during the provision of medical services by the doctor (medical institution) and the patient, such harm can be considered legitimate if the possible extent and circumstances of its occurrence are established within limits that do not contradict public morality and fundamentals of law and order (Tikhomirov A.V., 1996).
Surgery
Surgical treatment is called bullectomy. If a person is diagnosed with a giant bulla, then this is an indication for surgical treatment. Small bullae are difficult to treat surgically, and the effect of the operation is insignificant. Shortness of breath rarely improves.
Bullae that are not accompanied by clinical symptoms (shortness of breath) or complications (pneumothorax, suppuration) are not recommended to be removed.
Contraindications to bullectomy include continued smoking, severe cardiovascular disease, and diffuse emphysema with low compression of the surrounding lung tissue.
The indication for surgical treatment may be recurrent pneumothorax against the background of bullous changes. In this case, bullectomy and pleurodesis are performed simultaneously.
Emphysema
| Emphysema |
Emphysema is a chronic, progressive disease that relatively often leads to disability. It is believed that in the general population more than 4% of patients with symptoms of emphysema occur. According to autopsy data, it is recorded in deceased men in 60% and women in 30% of cases. This form of pulmonary pathology becomes especially dangerous with age and after 60 years it turns into one of the main leading clinical problems.
Emphysema belongs to a group of human diseases that are defined as chronic obstructive pulmonary diseases; This group of pulmonary pathologies, in addition to emphysema, includes bronchial asthma, chronic obstructive bronchitis, cystic fibrosis, and bronchiectasis. In clinical practice, difficulties often arise in the differential diagnosis of chronic obstructive bronchitis and emphysema, therefore chronic obstructive pulmonary disease is sometimes interpreted as an emphysematous or bronchitis variant. In contrast to the clinical and functional definition of bronchitis, emphysema, according to the recommendations of the European Respiratory Society, is considered from a pathoanatomical point of view as a destructive process of the elastic framework of lung tissue. However, it should be emphasized that such an approach to defining emphysema does not replace the etiological, clinical and radiological features of this pulmonary pathology. Many authors emphasize the imperfection of this definition of emphysema, always accompanying it with explanations regarding the meaning of the pathological destruction of elastic fibers of the lung tissue. It is known that the airways are fundamentally divided into two categories: bronchi and bronchioles. The distal part of the respiratory tract is represented by terminal bronchioles, which are part of the acinus, on the surface of the alveoli of which gas exchange occurs. Emphysema is defined as an abnormal enlargement of either all the constituent parts of the acinus, or a specific anatomical part of it. Abnormal enlargement of the acinus occurs due to the destruction of respiratory tissue. Hyperairiness of the respiratory tract can appear in a person during vigorous conversation, intense physical activity, or cold exposure to the respiratory tract, but an increase in air space is not considered as emphysema. Hyperairiness is also reversible during an attack of bronchial asthma; it regresses as soon as the signs of exacerbation of asthma disappear. Doctors, when describing the clinical picture of hyperairy lungs, sometimes use the term “vicarious emphysema.”
Thus, emphysema is characterized by a destructive process of elastic fibers of the lung tissue and the irreversibility of these anatomical changes.
In the specialized literature, the question of the role of age and gender in the development of emphysema is often raised. Indeed, in older age groups, especially after 60 years, emphysema is much more common than in younger people. However, it should be noted that the most aggressive risk factors that provoke the development of emphysema are long-term smoking, occupational hazards, infectious diseases of the respiratory tract, and long-term use of certain medications (steroid hormonal drugs, etc.). If we compare and compare the importance of each of the risk factors in the development of emphysema in humans, then age and gender will be in last place. A certain form of senile emphysema is identified, associating it with very advanced age and a number of concomitant diseases.
Over the past three decades, the problem of genetic predisposition to emphysema has been actively discussed. In 1965, Erickson described alpha-one antitrypsin deficiency, and this genetic phenomenon has become the subject of intense research to determine its role in the development and progression of pulmonary emphysema. The modern molecular biological concept is based on an imbalance in the proteolysis-antiproteolysis system. Alpha-one antitrypsin is the main inhibitor of serine proteases, which include trypsin, chymotrypsin, neutrophil elastase, tissue kallikrein, factor Xa and plasminogen. The PI (proteinase inhibitor) gene is located on the long arm of chromosome 14 (14q31-32), the product of this gene is the glycoprotein alpha-one-antiprisin. The PI gene is expressed in two types of cells—macrophages and hepatocytes; the tissue specificity of the inhibitor is associated with the function of the latter. The central place in the pathogenesis of emphysema belongs to the migration of neutrophils into the alveolar space, their infiltration of the bronchial wall and the high concentration of neutrophil elastase in the bronchoalveolar lavage fluid.
The highest concentration of alpha-one antitrypsin is found in serum and approximately 10% of its serum level is detected on the surface of airway epithelial cells. Inhibitor deficiency is associated with the intensity of the inflammatory process in the respiratory tract or is of a genetic nature. The main clinical manifestations of alpha-one antitrypsin deficiency are emphysema and juvenile liver cirrhosis. Delineated genetic cases of emphysema—sometimes referred to as essential—occur in young adults; this form is often combined with liver cirrhosis.
| Emphysema is defined as an abnormal enlargement of either all the constituent parts of the acinus, or a specific anatomical part of it. Emphysema is characterized by a destructive process of elastic fibers of the lung tissue and the irreversibility of these anatomical changes |
It was already indicated above that the most aggressive risk factors in the occurrence of emphysema are environmental pollutants, occupational hazards, smoking and recurrent respiratory infectious diseases.
Emphysema is, to a certain extent, an environmentally determined disease. A large amount of both experimental and clinical-epidemiological material has been accumulated, indicating the significant role of pollutants in damage to pulmonary structures, in the formation of a chronic inflammatory process of the respiratory tract and the occurrence of an imbalance in the proteolysis-antiproteolysis system. Among the pollutants, the most important are sulfur and nitrogen dioxides (SO2 and NO2), the main producers of which are thermal power plants and transport. When sulfur and nitrogen dioxides penetrate through inhalation, damage occurs to the membranes of the apical part of epithelial cells. Biological signals of this damage lead to the release of inflammatory mediators, leukotrienes, and a disruption occurs in the oxidant-antioxidant system. Depletion of the antioxidant system also plays an important pathogenetic role in the ongoing inflammation of the mucous membrane of the respiratory tract. Factors that lead to the development of emphysema also include black smoke and ozone. An increase in ozone concentration is associated with the use of freon in everyday life (refrigerators, household aerosols, metered aerosol medicines, perfumes). In hot weather, a photochemical reaction of nitrogen dioxide (a product of combustion of transport fuel) with an ultraviolet flux occurs in the atmosphere; the resulting ozone provokes inflammatory reactions in the mucous membranes of the respiratory tract. Increased ozone concentrations in large cities with a lot of traffic are associated with exacerbation of pulmonary and cardiovascular diseases. It should be noted that older people are more sensitive to pollutant effects and have a harder time with exacerbation of chronic diseases. The literature describes an increase in mortality, the cause of which was the high concentration of dioxides in the city’s air. Such cases were observed in England (London, 1948 and 1952), then over 4,000 people died within two weeks; in Belgium (1928), in the 50s, in many countries of Western Europe, outbreaks of pulmonary diseases occurred as a result of high concentrations of pollutants in the environment. In all environmental pulmonary epidemics described, the most sensitive were the elderly and young children.
There was a high rate of deaths among older people. The reasons for such a high sensitivity of the respiratory organs of elderly people to environmental factors should be sought in prolonged exposure to unfavorable environmental conditions, depletion of defense systems against the damaging effects of pollutants - and all this against the background of acquired chronic pulmonary diseases.
Smoking is perhaps one of the most aggressive factors in the development of chronic obstructive pulmonary disease. The development of emphysema is associated with the fact that tobacco smoke causes the migration of neutrophils, including the terminal part of the respiratory tract. Direct studies were carried out and the number of neutrophils was calculated using bronchoalveolar lavage before and after smoking. The number of neutrophils increases by several orders of magnitude and at the same time the concentration of neutrophil elastase increases. Another damaging mechanism in chronic smoking is associated with the accumulation of tobacco smoke tar elements in alveolar macrophages. Alveolar macrophages acquire a sandy color, which allows cytologists to isolate macrophages from a smoker from a wide variety of pathological processes in humans. Elimination of resin from macrophages is difficult, since it is not digested, is not eliminated, and only persists from the old and dying macrophage to the young phagocytic cell.
A large number of epidemiological studies have been conducted, on the basis of which it has been established that after 15–20 years of smoking, pulmonary changes of both a bronchodilator and emphysematous nature occur. The concept of a smoking person's index was introduced. It is derived by arithmetically calculating the number of cigarettes a person smokes per day, multiplied by 12 (the number of months in a year). If the index exceeds the number 200, that is, a person smokes more than 18 cigarettes per day, then pulmonary symptoms will certainly appear. It is believed that the life expectancy of a smoker is on average 10–15 years less than that of a non-smoker.
Smoking in Russia is very common. Epidemiological studies have been conducted that have revealed that men aged 20–50 years smoke in more than 70%, women in the range of 5-8%. It should be noted that in rural areas smoking is even more common, especially among men. The greatest adverse effect is achieved when cold and industrial factors are combined with smoking. In one of the studies of the Institute of Pulmonology, conducted among steelworkers at a Moscow automobile plant, signs of emphysema and bronchitis were identified in more than 30% of workers. The age of the men did not exceed 45 years. However, at the time of the examination, practically none of them had complaints about the respiratory system. This is one of the difficulties in early diagnosis of emphysema. A person does not subjectively feel his emphysematous disease for a long time. These patients begin to come to the attention of doctors when the disease becomes disabling and emphysema is combined with signs of chronic respiratory failure.
| One of the main difficulties in early diagnosis of emphysema is that a person does not feel his illness for a long time. These patients begin to come to the attention of doctors when the disease becomes disabling and emphysema is combined with signs of chronic respiratory failure |
Other risk factors include alcohol consumption, and repeated episodes of viral respiratory tract infection are of great importance.
Older people, who are so frequently diagnosed with emphysema, have the cumulative effect of several risk factors throughout their lives. The disease can develop rapidly and manifest as progressive shortness of breath, especially with a form of pulmonary pathology such as bronchiolitis obliterans.
Thurlbeck and Churg (1995) analyze in some detail old and new data on the pathological picture characteristic of emphysema. Morphometric studies of the size of the entrance to the alveoli indicate that in 94% of cases their size did not exceed 10 mm, while in emphysema the alveolar pores exceeded 20 mm. The alveolar wall is represented by vascular smooth muscle, the capillaries become thinner and empty. Elastic fibers are in the stage of degeneration.
The described morphological changes increase with age and, according to Thurlbeck, can serve as a hallmark of a person’s age. Degeneration of elastic fibers, emptying of capillaries, and a wide entrance to the alveoli lead to a decrease in the surface of actively functioning alveoli. Morphologically unchanged alveoli can be compressed by emphysematous changes, which ultimately plays an important role in disrupting the ventilation function of the lungs. In modern literature, the concept of a destructive index has been introduced. It is determined by three parameters: the presence of a certain number of alveoli with a destroyed wall; cuboidal epithelium lines the alveoli; there are classic emphysematous destructive processes affecting elastic fibers. For non-smokers this index ranges from 7 to 26%, while for smokers it exceeds 90%. The destructive index has large values in severe forms of emphysema and decreases in moderate and mild manifestations of the emphysematous process.
The anatomical classification of emphysema is based on the involvement of the acinus in the pathological process; There are proximal acinar emphysema, panacinar emphysema, distal emphysema and irregular emphysema.
In proximal acinar emphysema, the respiratory bronchiole, which is the proximal part of the acinus, is abnormally enlarged and destructured. Two forms of proximal acinar emphysema have been described: centrilobular and miners' pneumoconiosis. The centrilobular form of proximal acinar emphysema is characterized by changes in the respiratory bronchiole proximal to the acinus, which creates the effect of a central location in the lung lobe. It must be emphasized that the distal lung tissue is intact if the degenerative process has not progressed far. Centrilobular emphysematous areas are usually located mostly in the upper lobe; the anterior and posterior segments are more severely affected.
Miners' pneumoconiosis is characterized by a combination of interstitial fibrosis of the lungs with the development of focal emphysematous areas. The identification of this form of emphysema is based on the atypical fibrous process and its connection with the entry of mineral dust into the respiratory tract.
Panacinar emphysema has been described under various names: diffuse emphysema, generalized emphysema, alveolar or vesicular emphysema; it is characterized by involvement of the acinus in the process; the pathological process is relatively uniform.
It is believed that first the alveolar ducts and sacs are involved in the process, then they increase in size and become flat, and the line between the alveolar duct and the alveolar sac is blurred. The anatomical localization of panacinar emphysema mostly occurs in the lower lobes of the lungs, this is especially typical for severe emphysema.
Distal acinar emphysema is characterized by the involvement of predominantly alveolar ducts in the pathological process. The last anatomical type of emphysema is designated as irregular (irregular) and is characterized by a diverse enlargement of the acini and their destruction. It is often combined with a pronounced scarring process in the lung tissue, which is what is associated with the irregular nature of emphysema. A similar pathological process is observed in granulomatous pulmonary diseases (tuberculosis, sarcoidosis, pneumoconiosis, histoplasmosis and eosinophilic granuloma).
A special form of emphysema should be distinguished, which is known as the bullous form. A bulla is defined as an emphysematous area of the lung exceeding 1 cm in diameter. Reid identifies three types of bullae. The first type of bullae occurs regardless of the prevalence of emphysema. It is located subpleurally in the upper lobes of the lungs and has fibrous tissue at the entrance to the bulla. The second and third types of bullae occur with widespread emphysema. The second type is characterized by subpleural localization, while the third type is characterized by arbitrary localization.
Laennec brilliantly described a certain form of emphysema, which is now known as pulmonary interstitial emphysema; Historically, other terms have been used: subcutaneous emphysema, pneumomediastinum, pneumothorax, and others. This form of emphysema can occur in patients with bronchial asthma and complicate the course of the asthmatic condition during artificial and assisted ventilation, bronchoscopy, barotrauma, and placement of a subclavian catheter.
The clinical picture of emphysema does not have clear pathognomonic signs. In particular, this was one of the reasons for including the concept of this pathology in the group of chronic obstructive pulmonary diseases, which combines such related diseases as obstructive bronchitis, bronchial asthma and emphysema.
The clinical picture of obstructive bronchitis is especially similar to emphysema. However, there are certain differences on which differential diagnosis can be based; it to a certain extent influences treatment programs and the prognosis of the disease.
The main criteria for the differential diagnostic process are clinical signs and data obtained during functional tests. The clinical picture is dominated by shortness of breath, cough, sputum, and weight changes.
Shortness of breath in patients with emphysema develops gradually and, as a rule, begins to bother a person in the sixth or seventh decade of life.
Patients rarely report prolonged cough and sputum; this information often comes from family members. The emphysematous nature of shortness of breath belongs to a certain type, and during the period of exacerbation of the disease, with an accompanying cough, the face acquires a pink tint. In the English-language literature, the term pink puffers is used, thereby emphasizing the features of respiratory failure in patients with emphysema in contrast to patients with chronic bronchitis - blue bloaters (meaning diffuse blue cyanosis, literal translation - “blue color of smoked herring”). All authors who touch on the topic of shortness of breath in patients with emphysema emphasize its insidiousness: for a long time it does not manifest itself noticeably, gradually progressing, it turns into a real threat to human life.
The shortness of breath that occurs with obstructive bronchitis is mostly associated with a respiratory tract infection. It is known that bronchitis is functionally defined as a cough, which in the last two years of a patient’s life bothers him for three months a year; This emphasizes the close connection between the symptoms of bronchitis such as cough and shortness of breath.
In patients with emphysema, sputum is always produced sparingly and is mucoid in nature. It must be taken into account that with emphysema, the pathological process affects the terminal part of the respiratory tract, so little sputum is always released. And secondly - this applies to the mucoid type of sputum - with emphysema the bacterial inflammatory process does not dominate. An exacerbation of bronchitis is always accompanied by increased coughing and copious discharge of sputum, which is purulent in nature. Of course, the pathogen and the degree of its colonization in the mucous membranes of the respiratory tract play a large role in the occurrence of cough and the formation of the character of sputum. For practical purposes, it is necessary to pay attention to the appearance of a nonproductive cough and the cessation of sputum production. These symptoms indicate a severe exacerbation of obstructive pulmonary disease: on the one hand, a respiratory infectious process, on the other, the formation of respiratory muscle fatigue syndrome. Current guidelines consistently emphasize the avoidance of unnecessarily prescribed sedatives and antitussives, which can also contribute to mucus stasis in the airways, thereby helping to spread respiratory infections.
Patients with emphysema experience significant weight loss; They are, as a rule, thin and attract attention due to their large weight deficit. Such patients often avoid undressing in the presence of strangers and even doctors. Sometimes patients resemble cachectic people, and a slight technical difficulty arises when performing percussion and auscultation. Weight changes in patients with emphysema are associated with intense work of the respiratory muscles, which is aimed at overcoming the high resistance of the terminal airway. In the prognosis of the disease, great importance is attached to the functional state of the respiratory muscles - with the appearance of their fatigue syndrome, the disease always progresses, which immediately affects the worsening of signs of respiratory failure. Modern recommendations for the management of pulmonary patients pay attention to the assessment of the group of muscles involved in the act of breathing, the appearance of signs of paradoxical breathing, the synchronous participation of the diaphragm and abdominal muscles in the respiratory cycle (it is advisable to carry out the assessment in a sitting and lying position). In patients with emphysema and pronounced changes in the chest, as well as fatigue of the respiratory muscles in a horizontal position, intense work of the diaphragm is observed - patients are sometimes forced to sleep in a sitting position.
Patients with obstructive bronchitis experience approximately the same problems, especially during the period of progressive respiratory failure. However, they are not characterized by high weight deficiency, as for patients with emphysema.
External examination, percussion and auscultation also give the doctor the opportunity to identify a number of differential diagnostic signs. The chest in patients with emphysema is cylindrical in shape, the pulmonary sound over the entire surface has a box-like tint. The lower borders of the lungs are lowered by one or two ribs, the apices of the lungs protrude above the collarbones; on auscultation, breathing is sharply weakened; wheezing is not characteristic of emphysema, and a meager amount of it may appear during a cough test or as a tracheal sound at the height of forced expiration. In patients with chronic obstructive bronchitis, the clinical picture generally resembles that described above.
However, the appearance of wheezing, its increase in a horizontal position, different tones during forced exhalation and during a cough test - all this makes it possible to distinguish one form of obstructive pulmonary pathology from another.
In terms of the cardiovascular system, some differences are also noted. Thus, the formation of cor pulmonale is more typical for patients with chronic obstructive bronchitis, while in patients with emphysema these changes, if they develop, are already in the terminal stage of the disease. The difficulty of cardiac auscultation in patients with obstructive pulmonary diseases should be emphasized; Because of emphysema, heart sounds are difficult to hear, they are so muffled; auscultation is recommended to be performed in the epigastric angle, where the excited work of the hypertrophied right chambers of the heart is visually determined.
X-ray examinations of the chest organs are of great importance in the diagnosis of pulmonary emphysema, making it possible to identify its characteristic signs. It is always necessary to pay attention to the low position of the diaphragm dome and its flattening. When performing functional tests, you can find that the excursion of the diaphragm is noticeably reduced. These changes correspond to increased airiness of the pulmonary fields and an increase in the retrosternal space (Sokolov's sign); the cardiac shadow is narrowed and elongated (in this case, the figurative expression is “drip heart”); the pulmonary fields are depleted of vascular shadows; from the root of the lungs they quickly acquire a thread-like character and their shadows disappear towards the periphery of the pulmonary fields. Increased pulmonary pattern is more typical for areas of bullous emphysema. Computed tomography can significantly facilitate diagnosis by confirming hyperairiness, depletion of the pulmonary fields in the vascular pattern, as well as more clearly identifying bullae, their location and size. Emphysematous lungs indicate large disturbances in the ratio of ventilation and perfusion - such studies are carried out using radioisotope technology. In patients with chronic obstructive bronchitis, an X-ray examination of the chest organs generally reveals the above-described changes. However, attention is drawn to the high density of the bronchial wall, infiltration along their length - that is, a number of signs characterizing the inflammatory process in the bronchial tree.
In making a diagnosis of chronic obstructive pulmonary disease, a large role is given to the study of respiratory function. For emphysema, the most characteristic functional signs are a decrease in the elastic properties of the lungs, collapse of the distal airways, an increase in airway resistance, detected using general plethysmography, and an increase in dead space. The velocity indicators of the flow-volume curve are changed, but they are more typical for obstructive bronchitis. In modern pulmonology, inhalation tests with bronchodilators are common, allowing one to assess the reversible or irreversible nature of obstructive disorders. In patients with emphysema, the obstruction is persistent and irreversible, while in patients with obstructive bronchitis, a partial bronchodilator response is noted. In these two groups, a difference is revealed in the diffusion capacity of the lungs, which is impaired to a large extent in patients with emphysema. These changes may explain why hypoxemic disorders occur earlier in patients with emphysema. In patients with obstructive bronchitis, there is an early and persistent increase in pressure in the pulmonary artery system, which influences the appearance of characteristic blue cyanosis in this group of patients, while in patients with emphysema, pressure in the pulmonary artery remains at a normal level for a long time or increases with physical activity .
With the development of hypoxemia, polycythemic syndrome is formed in those suffering from obstructive pulmonary diseases, which is characterized by an increase in the number of red blood cells, high hemoglobin, low erythrocyte sedimentation reaction and increased blood viscosity. Erythrocytosis and blood hyperviscosity aggravate hypoxemic disorders, and with their appearance, signs of respiratory failure increase. During this period, cyanosis acquires a characteristic purple tint to the mucous membranes, tip of the nose, and extremities. The described changes are more typical for patients suffering from chronic obstructive bronchitis.
In these groups of patients, it is necessary to measure oxygen tension in arterial blood. Those patients whose oxygen tension in the artery is below 60 mm Hg should be placed in a special group. Art. - this is a sign of terminal respiratory failure, and such patients are indicated for long-term (more than 12-15 hours) oxygen therapy per day. It is also necessary to distinguish patients who have increased CO2 tension in the arterial blood - a hypercapnic group of patients; they do not require urgent therapeutic measures. Hypercapnia is associated with exacerbation of respiratory failure and the appearance of respiratory muscle fatigue syndrome. It is necessary to monitor blood gases in order to correctly build a treatment program and determine the prognosis.
In modern medical practice, the concept of disease biomarkers is becoming widespread. Of course, the appearance of certain symptoms forces patients to be divided into different groups: bullous emphysema, interstitial emphysema, genetic essential emphysema, and finally, lung diseases of a smoker, occupational pulmonary diseases. In clinical practice, there remains a significant group of patients who are treated as patients with chronic obstructive pulmonary disease. In this category, it is difficult to distinguish between the leading pathological processes associated with either obstructive bronchitis or the development of emphysema; in this regard, patients with bronchiolitis obliterans pose a particular difficulty.
There are no specific treatment programs for pulmonary emphysema and they do not differ significantly from those recommended in the group of patients with chronic obstructive respiratory diseases. However, more than 10 years ago, attempts were made to introduce human alpha-one antitrypsin replacement therapy. But this approach remained at the level of preclinical treatment programs and is currently not widely used in clinical practice. Manipulations in the proteolysis-antiproteolysis system come down to the administration of secretolytic, antioxidant agents and vitamins. None of these prescriptions have a direct effect on the proteolysis system. Much attention is paid to the long-term administration of acetylcysteine, as it reduces the production of free radicals, regulates the formation of secretions and has complexing properties.
In the complex treatment of patients with pulmonary emphysema, first place should be given to general measures that improve the quality of life of patients. Great importance is attached to quitting smoking. Modern studies devoted to the diseases of smokers have revealed extremely low activity of doctors when it comes to providing assistance to smoking patients; Doctors ask a formal question whether the patient smokes or not in less than 50% of cases; treatment programs are offered in general in 5-8% of cases. Success in the treatment of emphysema depends entirely on the doctor’s attitude. However, both the appeal of patients and their active identification raises the fact that preventive programs no longer play as effective a role as they could have played several years ago.
The drug program includes the prescription of bronchodilators, anticholinergic drugs, theophyllines and corticosteroids. The prescription of the first two groups (beta-two agonists and anticholinergic drugs) is more indicated for the treatment of patients with obstructive bronchitis than for patients with pulmonary emphysema. In clinical practice, these drugs, especially beta-2 agonists, are often prescribed due to the concomitant nature of pulmonary disease. In recent years, emphasis has been placed on long-acting beta-2 agonists (salmeterol, formoterol) and combined beta-2 agonists in combination with an anticholinergic drug (pheneterol + ipratropium bromide). This should be taken into account when it comes to older patients, since their cardiotoxicity (naturally, an undesirable effect) is less pronounced.
Preference should be given to theophyllines. However, when treating older people, the arrhythmic properties of theophylline may appear early. The low effect of theophyllines is observed when the FEV per second decreases below 1.5L. Preference is given to long-acting theophyllines, which allow a blood concentration of no higher than 15 g/L. The indication for the use of theophyllines is a violation of ventilation and perfusion, which is so typical for patients with emphysema.
Indications for the use of corticosteroids are quite controversial; more than 20% of patients with obstructive pulmonary diseases do not respond positively to therapy. It is necessary to take into account the myopathic effect of corticosteroids, which is extremely undesirable in patients with emphysema. The indication is the rapid progression of the disease, which cannot be stopped with the help of other drug programs. It is usually recommended to prescribe prednisolone at a dose of 15-20 mg with an assessment of effectiveness over the next three to four days. With emphysema, a person develops osteoporosis, which can be worsened by the use of corticosteroids. For the treatment of osteoporosis, vitamin preparations and especially vitamin D3 are recommended; in more severe cases, a course of calcitonin therapy is indicated. Physical programs are recommended for all patients with emphysema, especially chest massage, breathing exercises and teaching the patient kinesiotherapy.
Patients with emphysema may develop complications that will require special treatment measures. Pneumothorax is one of the most severe complications that threaten the patient’s life.
With the development of pneumothorax, antitussive narcotic drugs, installation of a drainage tube and connecting it to a cylinder with water, in which a negative pressure of 30 cm of water column is created, are indicated.
The development of modern thoracoscopic technology makes it possible to more often resort to the treatment of bullous emphysema using endosurgical methods. Literature: 1. Bennet C. and Plum F. Text book of medicine, 1996. 2. Thurlbeck W., Churg A. Pathology of the lung, 1995. 3. Samelchuk E. I. The role of hereditary factors in the occurrence of chronic pulmonary diseases. Dr. dis. M., 1997. 4. Heck LW et al. Bennet: Isolation, characterization, amino-terminal amino acid sequence analysis of human neutrophil elastase from normal donors. Anal. Biochem. 1985, 149, 153–62. 5. Timens W. et al. Extracellular matrix and inflammation: a role for fibroblast-mediated defective tissue repair in the pathogenesis of emphysema? Eur. Respira. Rev., 1997, 7, 43, 119–123. 6. Sandford AJ, Weir TD, Dp Pare P. Genetic risk factors for chronic obstructive pulmonary disease. Eur. Respir., J., 1997, 10, 1380–1391. 7. Samelchuk EI, Chuchalin AG Mis — sense mutation of alfa-1-antichymotrypsin and COPD. Lancet, 1993, 342:624.
Biomarkers of emphysema:
- high epidemiological prevalence, especially in older age groups (elderly);
- smoking;
- pollutants of the external and internal human environment;
- occupational hazards (miners, steelworkers, workers involved in textile production, construction workers (for the elderly with a history);
- genetic predisposition associated with the appearance of genes that disrupt the synthesis of protease inhibitors (emphysema theory - proteolysis - antiproteolysis);
- X-ray signs of hyperairy pulmonary fields, their depletion of vascular pattern, flat, low-lying dome of the diaphragm;
- ventilation disorders are caused by a decrease in the elastic properties of the lung tissue, an increase in the overall resistance of the respiratory tract;
- high levels of residual volume, dead space;
- minimal effectiveness of bronchodilators.