- Indications for tooth extraction
- Contraindications for removal
Once upon a time, tooth extraction was considered one of the most common dental procedures. However, today doctors have radically changed their approach to treatment and are trying to avoid it even in the most hopeless situations. Despite the fact that modern technologies make it possible to implant a tooth immediately after extraction, natural teeth are still considered the best option. Therefore, such an operation is performed exclusively for medical reasons, which are divided into urgent and planned. Urgent indications include situations when pathological processes occur in the soft or hard tissues of the oral cavity that pose a potential threat to the patient’s health. Planned appointments are those that can be postponed indefinitely, that is, until the next visit to the dentist.
Reasons for performing tooth extraction surgery
Indications for an operation that involves removing the incisor from the alveolar socket are divided into two groups:
- emergency;
- planned in advance.
Emergency indications for performing tooth extraction are:
- acute inflammatory processes of a purulent nature (including those spreading to bone tissue);
- severe damage of no functional significance;
- severe acute pain in the absence of opportunities for conservative therapy;
- damage to the dental crown that cannot be repaired by placing a filling or dental prosthetics.
Indications for planned tooth extraction are:
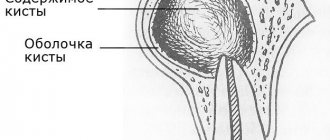
- the formation of basal cysts and the development of periodontitis in the tissues surrounding the incisor with impassable root canals;
- periodontitis, accompanied by severe tooth mobility;
- the presence of supernumerary, impacted or incorrectly located teeth that injure the mucous epithelium of the oral cavity, promote the development of inflammation, provoke pain, impair diction or interfere with food intake;
- tumor growths in jaw tissues;
- the presence of teeth that prevent prosthetics or orthodontic treatment.
How is a complex tooth extraction performed?
Complex wisdom tooth extraction is considered to be a case when the tooth cannot be removed with the simple application of forceps. As a rule, in such situations, access to the root of the tooth being removed is first created by cutting the mucous membrane and periosteum. Complex tooth extraction with an oblique or horizontal position is carried out in parts, for which a laser or a special saw is often used. You should not be afraid of this, since cutting a hard-to-reach tooth only shortens the time of its removal. After the procedure, the doctor smoothes the sharp edges of the bone wound, washes it with hydrogen peroxide or furatsilin, the mucoperiosteal flap is placed in place and fixed with sutures.
In complex cases, tooth extraction surgery does not have a uniform technique. How the doctor will act depends on the specific case.
Surgical technique
In modern dentistry, two tooth extraction techniques are used:
- simple;
- involving additional surgical procedures.
Simple removal is performed in cases where the coronal or root part of the damaged incisor is perfectly visualized and is well fixed in the forceps.
In such situations, the extraction procedure consists of the following steps:
- collecting anamnesis (the doctor makes sure that the patient has no contraindications to the procedure, carefully examines x-rays);
- anesthesia;
- peeling the gums from the enamel using a special tool;
- fixing the forceps on that part of the incisor that is located above the bone of the alveolar process;
- rocking it, accompanied by destruction of the ligamentous apparatus holding it in the alveolus;
- extraction of the tooth and all mobile fragments of bone tissue from the alveolar socket;
- removal of cysts, granulomas, sanitation of purulent foci in the area of the removed incisor (if indicated);
- treating the hole with antiseptics and anti-inflammatory drugs;
- suturing.
Indications for surgical tooth extraction may include:
- curvature of tooth roots, preventing safe tooth extraction;
- complete destruction of the part of the incisor rising above the alveolar process;
- increased fragility of the dental crown;
- incomplete eruption;
- its presence in the gum in a horizontal position.
Performing operations of this type may be accompanied by incision of the gum tissue, removal of the bone hiding the unerupted incisor using an osteotome or drill, sawing the crown into several parts and taking other measures to facilitate the extraction of problem teeth.
What is the typical tooth extraction process like?
When teeth are removed, local anesthesia is first administered. The doctor then removes about half a centimeter of gum tissue from the tooth. Then forceps are applied to the crown of the tooth being removed. When removing teeth in the upper jaw, the doctor presses on the forceps with his entire right hand. When removing teeth on the lower jaw, pressure is applied with the thumb of the right hand. The tooth is then dislocated to destroy the tissue that holds it in place. To remove single-rooted teeth, such as front teeth, rotational or pendulum-like movements are performed. When removing molars, pendulum-like movements are performed. The culmination of this action is the tooth extracted from the hole.
In what cases should teeth not be removed?
Contraindications to the operation are:
- acute infectious diseases;
- menstruation in women;
- hypertensive crisis, severe arrhythmia and other cardiac disorders;
- I and III trimesters of pregnancy;
- taking medications that reduce blood clotting;
- hemophilia and other blood diseases;
- epileptic seizures;
- schizophrenia and other mental illnesses.
If the listed pathologies and conditions are identified, the issue of tooth extraction is considered on an individual basis.
Contraindications for removal
This operation has no absolute contraindications, however, there are situations when, if possible, it is recommended to postpone it for some time. These include acute infectious, inflammatory and cardiovascular diseases in the acute stage, pregnancy, central nervous system lesions, malignant tumors, and circulatory disorders. If it is impossible to delay removal, the doctor must evaluate the patient’s condition and select appropriate medications and surgical methods for him. All manipulations are best carried out in a hospital setting, so that if any serious complications occur, the patient can be provided immediate assistance.
Features of hygienic care after surgery
For patients undergoing surgery to remove one or more teeth, it is recommended:
- stop eating food for 2.5 hours;
- do not chew food on the side of the postoperative wound until it is completely healed;
- temporarily stop consuming too hot drinks and food;
- refrain from brushing for 1.5 days;
- give up active physical labor for 3 days.
If complications develop (the appearance of prolonged bleeding, inflammatory processes, purulent discharge, etc.), you must immediately contact specialists at a dental clinic and undergo a course of therapy according to the regimen they have developed.
Indications for removal of primary teeth in children
At the age of 5–6 years, temporary teeth begin to fall out, giving way to permanent teeth. But sometimes you have to resort to removing a temporary tooth in the dentist’s chair. Here are the main indications for the removal of temporary teeth:
- Advanced caries. If a tooth is so damaged that it cannot be restored, the doctor decides to remove it.
- Cyst at the base of a temporary tooth.
- The temporary tooth becomes loose but does not fall out, injuring the gum tissue and causing inflammation.
- The temporary tooth does not fall out for too long, preventing the normal growth of the permanent tooth.
- Serious tooth injury - chip or crack, root fracture.
- Phlegmon, periodontitis, sinusitis.
Nerve removal
Removal of the nerve is carried out in the treatment of advanced caries, injuries, and prosthetics. The coronal part is preserved.
Types of pulp extraction:
1. Vital - the pulp chamber is opened, the doctor expands and cleans the canals. Medicines are administered to relieve the inflammatory process. A temporary filling is installed. At the next visit - permanent.
2. Devital – a drug is installed on the pulp tissue, which causes the cessation of its activity and a temporary filling. After a few days, the pulp is removed and the tooth canals are cleaned. Then a permanent filling is installed.
Planned indications.
There are a number of reasons why tooth extraction is inevitable, but the procedure can be postponed for a while and carried out when it is convenient for the patient.
Such indications include:
- chronic periodontitis outside the acute stage (if it is impossible to carry out therapeutic treatment of the tooth)
- tooth root cracks
- chipping of the tooth wall deep under the gum
- severe destruction of the crown part of the tooth by caries (if it is impossible to restore it with either a filling or an artificial crown)
- tooth root caries
- mobility of teeth III-IV degrees with periodontitis
- orthodontic indications (to correct bite)
- supernumerary, incorrectly positioned and impacted (not erupted) teeth
- teeth that injure surrounding soft tissues when it is impossible to move them (for example, wisdom teeth)
Types of procedure
The method of removing a molar, incisor or canine depends on the patient’s diagnosis and his response to conservative therapy. Types of surgical intervention:
- complete – the doctor removes the entire dental unit along with the roots
- resection – removal of the root apex with granuloma, cyst. The remaining roots are preserved and can be used for restoration or prosthetics
- hemisection—the doctor removes 1 affected root. The dental crown is preserved.
In addition, there are concepts of “simple” and “complex” removal. The latter involves extraction of a multi-rooted molar (wisdom tooth) with possible suturing.
Emergency indications.
Urgent tooth extraction is required if it has caused the development of:
- acute purulent inflammation spreading to the bone (periostitis, osteomyelitis)
- cellulitis or abscess of surrounding soft tissues
- sinusitis (inflammation of the paranasal sinuses)
- lymphadenitis (inflammation of regional lymph nodes)
if the tooth is not subject to conservative treatment or does not represent functional value, and also
- for severe toothaches when adequate treatment is impossible
- with a longitudinal tooth fracture
- in case of a fracture of the coronal part with exposure of the pulp, if the crown cannot be restored by filling or orthopedic treatment.
Anesthesia
Our goal is to make any oral procedure as comfortable as possible for the child. To do this, we can use any of the methods of pain relief in dentistry accepted in the world today:
- topical anesthesia (applying the drug to the gum);
- local anesthesia (injection of anesthetic using a carpule needle);
- in some cases, xenon-oxygen anesthesia is used (precedes local anesthesia to reduce anxiety).
Indications for removal of permanent teeth in children
Permanent teeth in children are rarely removed. This usually results from advanced caries with complications and serious inflammatory processes. In addition, there are the following indications:
- Advanced caries. If a tooth is so damaged that it cannot be restored, the doctor decides to remove it.
- Phlegmon, periodontitis, sinusitis.
- Cyst at the base of a permanent tooth.
- An unerupted tooth that cannot develop.
- Serious injury to a permanent tooth.
- Removal for orthodontic indications.
Healing process
If there are no complications, then after tooth extraction, complete healing of the gums occurs within 4 months in the following order:
- On the first day after surgery, a blood clot forms in the wound, which is necessary for the further healing process. The wound should not be disturbed with the tongue or rinsed.
- On the third day, a thin layer of epithelium forms. It is easily damaged, so you should brush your teeth carefully and avoid chewing hard food on the side of the extracted tooth.
- On days 4-8, the blood clot is actively replaced by connective tissue. By this time, there should be no open wound on the surface of the gum.
- On days 14-16 after extraction, the wound is completely overgrown with epithelium, the edges of the gums shift, instead of connective tissue, bone tissue begins to form in the socket.
- After 2-3 months, the process is completely completed, young bone tissue fills the entire hole.
- At 4 months, the bone tissue acquires the same structure as in the upper and lower jaw.
Complications arise if the wound becomes infected due to the doctor’s fault during surgery (ingress of pus, pieces of carious teeth) or due to the fault of the patient who did not follow the recommendations for care in the postoperative period. In these cases, gum healing is slower and accompanied by pain.
In advanced cases, the formation of abscesses and phlegmons with the threat of blood poisoning is possible. Therefore, if the pain in the wound does not subside after a few days, and the gums are inflamed, you should consult a doctor.
Timofeev volume 1-3 / volume 1 / 03. TEETH REMOVAL / 3.1. INDICATIONS AND CONTRAINDICATIONS FOR TEETH EXTRACTION
3.1. INDICATIONS AND CONTRAINDICATIONS FOR TEETH EXTRACTION
♦ Indications for tooth extraction
Despite the successful development of therapeutic dentistry, tooth extraction is the most common surgical procedure. More than 90% of operations performed in a clinic involve tooth extraction.
Conservative treatment methods
various forms of complicated caries - pulpitis, periodontitis - cannot be considered perfect. Despite the external well-being, baked teeth in a certain percentage of cases continue to be sources of chronic infection for a number of years and are the cause of the development of various odontogenic inflammatory processes of both soft tissues and bones of the maxillofacial area. A feature of odontogenic foci of inflammation is that defects in the hard tissues of the tooth, which are the entrance gates of infection, are not compensated naturally. This causes constant additional infection of not only the tissues of the maxillofacial area, but also the entire body, contributing to the formation of foci of chronic infection. A kind of dynamic balance is established between such a focus of infection and the patient’s body. It can be disrupted as a result of a decrease in the immunological reactivity of the patient’s body or changes in the odontogenic focus (virulence or the number of bacteria, if the pyogenic membrane surrounding the infectious focus is damaged).
The elimination of chronic foci of inflammation during the therapeutic treatment of periodontitis does not occur immediately after completion of root canal filling, even if the treatment is complete. In 22% of patients, odontogenic foci of chronic inflammation disappear after 4-8 months, in 68% - only 1-2 years after completion of dental treatment, and in other patients at a later date (V.I. Groshikov, 1966; A.I. Rybakov, 1976, etc. - Many authors indicate that certain methods and terms of treatment of dental diseases are violated (A.I. Rybakov, 1976; N.F. Danilevsky et al., 1982, 1988; A.I. Marchenko and al., 1988, 1989, etc.). Foci of open infection turn into closed, undrained ones, which serve as a source of sensitization and chronic sepsis in the patient’s body. As a result of chronic intoxication, odontogenic diseases of various organs and systems (heart, kidneys, bones, nervous system) can develop.
Indications for tooth extraction should be divided into absolute (urgent)
and
relative (planned).
For urgent (urgent) tooth extraction
are resorted to if in the periodontium, despite previously carried out conservative treatment, the inflammatory process does not subside, but intensifies. That is, acute purulent (exacerbation of chronic) inflammation develops in the periodontium, which is the source of the development of inflammation in the bone, sinusitis, perimandibular inflammatory infiltrate, abscesses and phlegmon, lymphadenitis. Tooth extraction is resorted to when there is a complication of difficulty in the eruption of wisdom teeth, if the latter do not have room for eruption.
It is necessary to remove a tooth when cystic forms of some tumors of the jaws (ameloblastoma, etc.) and radicular cysts suppurate, when the tooth cannot be preserved.
In case of fractures of the lower jaw, if the tooth is in the fracture line, there may also be a need for urgent tooth extraction. Indications for the removal of teeth located in the fracture line will be discussed in more detail in the corresponding chapter of the manual.
Planned tooth extraction
carried out according to the following indications:
• chronic granulating and granulomatous periodontitis, which, as a result of ineffective conservative treatment, remains a focus of chronic infection in the patient’s body; the latter cannot be eliminated by using other surgical methods of periodontal treatment - resection of the root apex, coronary-radicular separation, replantation, hemisection and amputation of the tooth root;
• complications associated with dental treatment (perforation of the tooth cavity or its root, breakage of an instrument in hard-to-reach areas of the tooth, etc.);
• the impossibility of medicinal treatment of a tooth when a significant part of its crown is destroyed, and the root of the latter cannot be used for prosthetics;
• incorrectly located single teeth in the dentition, which cause constant injury to the mucous membrane of the cheek, tongue, pterygomaxillary fold, especially if post-traumatic erosions and ulcers occur; Converging, diverging and supernumerary teeth that interfere with the manufacture of dentures;
• tooth mobility of the third degree and teeth protruding due to the lack of antagonists (Popov-Godon phenomenon);
• single teeth that prevent the stabilization of a removable denture;
• to eliminate malocclusion during orthodontic and surgical treatment;
• teeth that disfigure the patient’s appearance (especially when smiling);
• can sometimes be associated with phonation defects, when the presence of one or more teeth prevents the correct pronunciation of sounds;
• in the presence of tumors of the alveolar process, in some cases it is necessary to remove teeth to gain access to radical surgical intervention;
• if a child is born with erupted milk teeth (usually the lower incisors), they must be removed as they interfere with breastfeeding (if they cannot be covered with a protective plate);
• baby teeth, which cause inflammatory diseases, which prevents the involvement of the rudiments of permanent teeth in the inflammatory process and the development of purulent lesions of the jaws and perimaxillary soft tissues;
• removal of a baby tooth can be carried out for the purpose of timely eruption of a permanent tooth;
• destroyed lower permanent sixth teeth in children for the correct eruption of the lower seventh tooth;
• removal of a baby tooth may be indicated when it becomes mobile, resulting from root resorption or when resorption slows down and the root is exposed.
♦ Contraindications to tooth extraction
Absolute
There are no contraindications to tooth extraction, however, in some diseases and physiological conditions, the operation should be temporarily postponed.
Tooth extraction in these patients should be performed after appropriate preparation. Temporary (relative)
contraindications to tooth extraction surgery are:
♦ cardiovascular diseases (hypertension during a crisis, coronary heart disease with frequent attacks of angina at rest, atrial fibrillation, paroxysmal tachycardia, pre-infarction state, the first 3-6 months after myocardial infarction, rheumatism, aseptic endocarditis during an exacerbation, severe cardiac decompensation activities, etc.);
♦ kidney diseases (acute glomerulonephritis, renal failure);
♦ diseases of the pancreas (acute pancreatitis, hyper- and hypoglycemic coma);
♦ infectious hepatitis (acute and in the acute stage);
♦ blood diseases (leukemia, agranulocytosis, hemorrhagic diathesis - hemophilia, thrombocytopenia and other conditions that occur with hemorrhagic symptoms);
♦ hypovitaminosis (C-vitaminosis);
♦ acute respiratory tract diseases (flu, acute respiratory infections, bronchitis, pneumonia);
♦ acute infectious diseases (diphtheria, whooping cough, measles, scarlet fever, dysentery, tuberculosis, etc.);
♦ diseases of the central nervous system (meningitis, encephalitis, acute cerebrovascular accidents - stroke);
♦ mental illnesses during the period of exacerbation (epilepsy, schizophrenia, manic-depressive psychosis, etc.);
♦ pregnancy (1-2 and 8-9 months due to the risk of miscarriage or premature birth);
♦ acute radiation sickness;
♦ radiation therapy for tumors of the maxillofacial localization;
♦ acute inflammatory diseases of the oral mucosa and pharynx (stomatitis, gingivitis, tonsillitis);
♦ teeth located in the area of a malignant tumor (cancer, sarcoma) or hemangioma;
♦ milk teeth in adults when they are not replaced by permanent teeth.