Chief editor of the site:
Snitkovsky Arkady Alexandrovich
Chief physician of the professorial dentistry “22 Century”, dentist, orthopedic dentist
Author of the article:
Scientific team of dentistry “22 Century”
Dentists, candidates and doctors of medical sciences, professors
Materials and production of crowns
Artificial crowns are permanent prostheses in the form of caps that restore the anatomical shape of the tooth, chewing and aesthetic functions of severely damaged hard dental tissues. When they are manufactured in a dental laboratory, various materials or combinations thereof are used. They have a long history of use in dentistry: the first mentions date back to the 18th century.
What is a dental crown
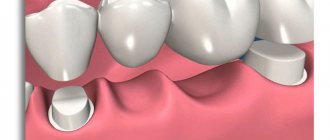
A crown is a type of dental prosthesis, non-removable, completely or partially covering the visible part of the tooth. Sometimes it is part of a larger prosthesis, such as a bridge. Crowns are distinguished:
- orthopedic. Replenish the missing part of the tooth crown. These include equatorial, three-quarter (for premolars), half-crowns (protect part of the vertical surface and the cutting edge);
- full clinical. Like a cap, they cover the entire stump of the tooth.
- stump, fenestrated, crowns with a pin are placed when more than 80% of tooth decay occurs, so they are often classified as pin structures.
To ensure that the crown does not interfere with the closure and active movement of the jaw, it is made according to the shape of the tooth, with a tight coverage of the neck without immersing more than 0.2 mm in the gum pocket. “Parts” for this type of fixed prosthetics are cast from metals, alloys, porcelain, and plastic. There are combined dentures, when a material different from the base is used for lining.
An inlay is first installed under the crown. Happens:
- straight (direct), made in the mouth, used when the tooth has 3 out of 4 walls left. Externally, it is a screw or pin that is inserted into the canal with a filling;
- indirect (indirect), an impression is made, and the inlay is cast from it in the laboratory.
The pin cult inlay is considered more reliable (and expensive); a ceramic inlay is placed under ceramic dentures.
Dental crown
Metal
This is a completely metal structure that fits over adjacent teeth and replaces the lost tooth. Products are made of gold, silver, aluminum, titanium, cobalt-chrome alloy and other combinations.
The models are strong and durable, they can withstand any load, do not crack or deform even when chewing hard food. Such prostheses have one drawback - they are hopelessly outdated.
A metal crown looks unattractive and immediately reveals its artificial origin, so it should not be installed in the smile area. The maximum for which it is suitable is the chewing zone, but for these purposes there are more practical and visually aesthetic types of prostheses. In addition, metal can provoke an off-taste in the mouth and oxidize.
In what cases is a crown placed on a tooth?
Purpose of artificial crowns:
- replenish lost tooth tissue;
- restore its damaged surfaces.
They are made when it is impossible to restore a tooth by filling or placing inlays, i.e. it has already been destroyed by 60% - 80%. Protective “caps” are used for certain diseases of the jaw, oral cavity, and soft tissues. For example, with arthrosis of the TMJ, a prosthesis is indicated to protect teeth from abrasion (wear) while restoring the size of the jaw opening.
Crowns are also retaining elements that secure bridges or removable dentures; they can level the surface of incorrectly positioned teeth with congenital defects of hard tissues (hypoplasie). Quite often, dentures are used to cover stained, discolored teeth due to caries and teeth with or without dead pulp.
Indications for tooth replacement with artificial crowns:
- Pathology of hard tissue, spreading over an area of 50 to 80%: caries;
- wedge-shaped defects (for example, a part broke off as a result of injury);
- pathological abrasion, for example, due to pathological clenching of the jaw (bruxism);
- hypoplasia (congenital anomaly, partial or complete absence of enamel);
- fluorosis (softening of hard tissues due to excess fluoride);
- erosion (destruction of enamel and dentin).
TERMS AND ACCEPTED ABBREVIATIONS
Personal data (PD)
– any information relating to a directly or indirectly identified or identifiable individual (subject of personal data);
Processing of personal data
– any action (operation) or set of actions (operations) performed using automation tools or without the use of such means with personal data, including collection, recording, systematization, accumulation, storage, clarification (updating, changing), extraction, use, transfer (distribution, provision, access), depersonalization, blocking, deletion, destruction of personal data;
Operator or organization
– a state body, municipal body, legal entity or individual, independently or jointly with other persons organizing and (or) carrying out the processing of personal data, as well as determining the purposes of processing personal data, the composition of personal data to be processed, actions (operations) performed with personal data;
Distribution of personal data –
actions aimed at disclosing personal data to an indefinite number of persons;
Providing personal data
– actions aimed at disclosing personal data to a certain person or a certain circle of persons;
Blocking personal data
– temporary cessation of processing of personal data (except for cases where processing is necessary to clarify personal data);
Destruction of personal data
– actions as a result of which it becomes impossible to restore the content of personal data in the personal data information system and (or) as a result of which material media of personal data are destroyed;
Depersonalization of personal data
– actions as a result of which it becomes impossible to determine the ownership of personal data by a specific subject of personal data without the use of additional information;
Automated processing of personal data
– processing of personal data using computer technology;
Personal Data Information System (PDIS)
– the totality of personal data contained in databases and the information technologies and technical means that ensure their processing;
Patient
– an individual who is receiving medical care or who has applied for medical care, regardless of whether he has a disease or his condition;
Medical activities
– professional activities in providing medical care, conducting medical examinations, medical examinations and medical examinations, sanitary and anti-epidemic (preventive) measures.
Attending doctor
– a doctor who is entrusted with the functions of organizing and directly providing medical care to a patient during the period of observation and treatment.
Contraindications for installation
The main contraindication to the use of a fixed prosthesis is considered to be poor oral hygiene. Over time, plaque may form around the “cap,” which damages the periodontium and intensifies caries. Therefore, first, teeth are cleaned, damaged teeth are removed, carious cavities are filled, and foci of inflammation are treated. Only then can the crown be installed.
Temporary contraindications also include:
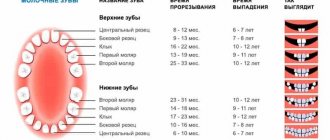
- age up to 16-18 years (individually, they look to see if the jaw continues to grow and the roots of the teeth continue to form);
- severe health condition (heart attack, ischemia, hypertensive crisis).
Absolute contraindications:
- Completely healthy teeth (intact), when they do not serve as support for devices or dentures.
- Pathological tooth mobility of the 3rd degree (mobility with an inclination, the tooth can rotate 360 degrees).
- Incurable infection in the periodontal area.
Types of products depending on coverage area
According to the classification of artificial crowns based on the area of tooth coverage, there are full and partial crowns. The most popular type is the full design. The choice of product largely depends on the group of teeth on which the crown will be installed, as well as on how badly they are damaged.
The stump crown is designed for installation on an almost completely destroyed tooth. This design is characterized by the fact that it is disassembled and reassembled. It can be made from various anti-allergenic materials. The fixation device combines a pin, an artificial tooth root and the crown itself.
The telescopic crown combines the supporting and outer parts. The design secures removable and fixed dentures, as well as certain maxillofacial devices.
Partial crowns are designed to replace the sides of teeth. It is designed to cover areas affected by caries, and is also used in cases of pathological abrasion of teeth. In some cases, it is used in the process of treating various pathologies. A half-crown covers only half of the tooth and is installed on the facial surface of the incisors and front teeth. Caries under an artificial crown is not noticeable and somewhat slows down its development.
Veneer crowns, which are made of plastic or porcelain, are very popular. Sometimes metal-free ceramics are used to make veneers. Unlike all other designs, they are aesthetically pleasing and more attractive.
Which crown is better to put?
Based on the materials used, the following types of crowns are distinguished.
Sitall
Crowns made of glass-crystalline materials are biologically inert, i.e. do not cause adverse clinical manifestations. Dentures resist the chewing load well, are quite elastic, and have increased resistance to the corrosive effects of aggressive agents. The main disadvantage is fragility. Recommended for allergy sufferers and chronically ill people (due to the consumption of a large number of medications, they should avoid anything that can provoke an allergy or cause a rejection reaction).
Porcelain (ceramics)
Standard porcelain “caps” are made with a stably fixed or separate metal pin (the second option is more convenient). A more expensive option is custom-made prostheses based on a platinum matrix. After 2 annealings, a stage of shape correction between them, the individual characteristics of the teeth (cracks, stains) are imitated on the surface. Then they are tinted with majolica glazes, securing with another annealing. Then the “cap” will look natural.
Porcelain crowns
The main disadvantages of porcelain fixed dentures:
- fragility;
- poor marginal fit;
- abrade the surface of antagonist teeth.
They are chosen by people who have high aesthetic requirements for the oral cavity (show business). Ceramic dentures are also used for those who cannot undergo restoration with a composite. If the occlusal load is distributed unevenly, the dentist will suggest a different material.
Metal
More than 500 alloys are used in dentistry, but most metal fixed dentures are made of chromium-nickel or silver-palladium alloy, as well as 900 gold with the addition of copper, silver, and platinum as a ligature.
Metal “caps” are resistant to alkali and acid (in small concentrations), have high wear resistance, are moderately elastic, and are relatively biologically indifferent. The fashion for the “gold tooth” is back. Metal prostheses are durable products that do not require special attention. The retention time of the properties of a metal crown depends on the alloy.
Zirconium dioxide
These are the most popular of all fixed types of prostheses. Zirconium oxide (or dioxide, in the formula there are 2 oxygen molecules per molecule of zirconium) is chosen by public figures. The process of making a “cap” is labor-intensive, using computer modeling, so the product is expensive. This is a category of elite prosthetics.
The crown is durable, its color and transparency are very similar to a real tooth. In terms of all the characteristics of medical implants (bioinertness, resistance to acid-base influence, elasticity) it is one of the best.
There are 2 types of crowns:
- with the application of ceramics, when metal is used as a base;
- without porcelain, then the desired shade is manually applied to it.
Advantages of zirconium fixed prostheses:
- Making fairly thin crowns with minimal grinding (this way the teeth remain alive).
- Accuracy of fit (computer modeling is used).
- The service life of crowns is from 10 to 20 years.
- High aesthetics. In terms of transparency and structure, they best match natural teeth.
- Strength. They are made for both front and chewing teeth.
- Biocompatibility.
- High precision in the manufacture of crowns allows you to achieve the tightest possible fit, avoiding the inflammatory process and the development of caries.
Metal ceramics
This is a good alternative to porcelain crowns, since metal-ceramic prostheses are characterized by:
- increased strength;
- better fit at the edges.
Metal ceramics
A metal alloy is used for the base, and a ceramic mass is applied to it. The best base is gold, in which case the base is thin, freeing up more space for ceramics. The metal will not show through the porcelain - this makes your smile look more natural. But there is a nuance: it is highly undesirable to install several fixed dentures (or a base with ceramics) made of different metals. For installation, deep preparation is used only on the vestibular surface (this is the side of the tooth turned towards the lips and cheeks) to mask the frame of the prosthesis.
Contraindications to installing metal-ceramic crowns on teeth:
- Teeth with thin crowns, when there is a risk of pulp damage.
- Deep blocking or wearing away bite.
- Pathological abrasion of tooth tissues.
- Parafunctions of the masticatory muscles, in which there is high muscle excitability, bruxism, and lateral displacement of the jaw.
Please note: it is better to avoid metal-ceramic crowns if you have marginal periodontal diseases, because Patients regularly experience functional overload of teeth, which leads to exacerbation of inflammation and deepening of the destruction process.
Metal-plastic
The second name for “caps” is combined, because Composed of plastic, composite, porcelain. These are temporary “caps” since the service life usually does not exceed 3 years. Plastic deteriorates over time under the influence of acids and alkalis, and can be colored with natural food dyes (wine). Summary: not bad, as a temporary option (there are situations, for example, injury, accident, but tomorrow you need to speak, be at negotiations).
Plastic
With good aesthetic properties, a plastic fixed prosthesis is inferior to its analogues in strength. It is not used to restore thin or flat incisors, with a deep or receding bite, pathological abrasion of teeth, or some dentition defects. This type of crown should not be placed on people with allergies.
Fixed dentures are made in 2-3 layers on an interpenetrating polymer mesh. They are recommended for prosthetics for children, during the correction of dentoalveolar anomalies, during periods of primary and mixed dentition.
Temporary crowns made of plastic
Main types of dentures
This is the name given to custom-made orthopedic structures that replace lost teeth. They are installed with the aim of restoring the aesthetic appearance and chewing function, as well as eliminating diction disorders.
Based on the type of fixation in the oral cavity, there are three main types of prostheses:
- non-removable – designed to replace several missing dental units (bridges) or restore a damaged tooth (crowns, inlays, veneers);
- conditionally removable - can only be removed by a specialist for maintenance or repair, attached to pins implanted in the jaw;
- removable - products made of metal, plastic, which are fixed with different types of fastenings to healthy teeth or with the help of special glue in case of complete edentia. Constructions of this type are divided into complete and incomplete in terms of volume of replacement of dental units.
Complete dentures
Designed to restore teeth when they are completely missing, they are made of hypoallergenic acrylic plastics. They consist of a base adjacent to the gum and crowns attached to it. A well-made artificial upper jaw is held in place well by negative pressure between the gum and the denture bed. The lower denture, as a rule, is less well fixed, so dentists recommend additionally using special adhesives.
Complete denture
Partial
They are installed in the presence of supporting dental units, correcting included or end defects. Metal, plastic, acrylic in various combinations are used in production. Modern orthopedic dentistry offers several options for partial structures that are fixed with locks, clasps, and other types of fasteners. The chewing load is evenly distributed both on the jaw tissue and on the prosthesis.
How to install crowns on a tooth - all stages
Let's look at the stages of installing a crown on a tooth in more detail.
Diagnostics
Before making a fixed denture, a clinical evaluation of the tooth is performed. Using a dental mirror, tweezers and a probe, the doctor:
- determines the degree of crown destruction, the severity of the equator:
- records the presence of seals;
- determines the relationship of the prosthetic tooth with adjacent teeth and antagonist teeth;
- studies the condition of the periodontium and the degree of tooth mobility.
To exclude contraindications (neoplasms, inflammatory processes), the dentist may also refer the patient for an x-ray.
Preparing for installation
The tooth under the denture should be as healthy as possible, i.e. cleared of plaque, caries, sealed if necessary, and the inflammatory process is eliminated. In this case, the dentist may recommend removing the nerve, but the tooth without the nerve dries out under the prosthesis and becomes less durable. Underneath it, even with perfectly filled canals, 1 in 10 (statistics from The American Dental Association (ADA)) develops an infection in the periodontium. Over time, pain will appear in this place, the “cap” will begin to dangle, and secondary caries will develop underneath it.
Remember: the doctor must do a cold test on the nerve (usually a cold stream of water is used for this). The nerve is removed if the pain does not go away after a few seconds.
After removing the nerve and filling the canals, everything unnecessary is removed from the tooth (pin, fillings, caries). The thin walls are shortened, forming a platform for the inlay, and the edges of the treatment are smoothed so that they do not scratch the tongue or cheek when the inlay is installed. When turning, the tooth is given the shape of a cylinder, and the cavity inside is oval-shaped - this increases the reliability of fixation of the inlay.
Grinding a tooth for a crown
Taking an impression, choosing a color
To obtain an impression use:
- standard impression trays with perforations to hold the impression material in the tray;
- impression materials (for example, Algmat).
The taken impression is called a “negative”. When it is cast with hard plaster, they will receive a “positive” - an exact model of the teeth.
An inlay pin is placed in the prepared tooth, then an imprint is taken using silicone mass (always together with adjacent teeth). Another impression is made of the entire jaw and antagonist teeth. Quality criterion: the impression must accurately reproduce the position of prepared and unprepared teeth, the relative position and distance between them, as well as the position of soft tissues.
The average production time for an inlay is a week. Before cementing the inlay, the pins are cut to the same level as it. They try the inlay on the tooth, check the tightness of the fit, and then cement it. It is clear that this is not construction cement, especially not a cement mortar with sand. This is a special glass ionomer cement for dentistry.
After 20-25 minutes, the excess is removed, a retraction thread is laid around the perimeter of the tooth to slightly move the edge of the gum. Then in the future the “cap” will not hang over the gum. Then the tooth is polished and smoothed again so that the fit of the fixed prosthesis is as tight as possible and the remainder of the tooth is not destroyed. A silicone impression is then taken to create the crown.
Temporary composite “caps” are made that will protect the gums until the next visit. They are installed with temporary cement. Now you can choose the color of the future prosthesis.
To do this, they use a “color key”, which contains on average about 15 samples. The sample is compared with the teeth, choosing the color closest to them in daylight, neon and artificial light (!). It is better to meet with a technician for this, because... a real tooth has a color transition from light to dark, more transparent at the edges. Only a technician can correctly determine:
- color;
- tonal ratio (light – dark);
- color intensity (saturated – pale);
- color (yellowish – reddish).
They come to the dental technician without makeup, wearing uniform, gray clothes.
Crown making and fitting
In a modern dental clinic, crowns are made using the best impression materials and computer modeling, so there is no fitting stage. If the clinic is budget (but this does not mean that bad doctors work there), or several prostheses are made, fittings are carried out. To put a “cap”, it is placed on temporary cement and the quality of work is checked.
Making crowns
The process of installing a crown on a tooth
The tooth is cleaned of the remains of temporary cement, a retraction thread is laid so that when the “cap” is installed, moisture does not get on the tooth. They place a crown on the tooth and check the tightness of the edges. They are fixed with cement (the excess is, of course, removed).
The quality of the installation is checked using dental floss: it should pass between the teeth under tension and make a loud click. Then food remains will not remain between the teeth.
How to place crowns on implants
Installing a crown on an implant is slightly different from installing a crown on a tooth; it is recommended for severely damaged teeth. After diagnosis, the dentist prepares the oral cavity for implantation. This is a titanium alloy screw that is screwed into the bone. It has a conical head that imitates a tooth. This is where the “cap” will be put on.
Just like with conventional crowns, the inflammatory process and caries are first treated. Then an implant is installed into the bone or tooth root (an anesthetic injection is given first), which will take root in 5-6 months.
Please note: as the healing time decreases, the risk of implant failure increases.
Next begins the stage of installing gum formers, which are required for uniform growth of soft tissue around the implants, taking into account future crowns. Impressions for dentures are removed after 2 weeks. First, using a dental key, the formers are removed and transfers are installed, which will remain in the impression and become the basis for attaching the implants.
An impression is taken using silicone impression material, as when installing conventional crowns. Then a plaster model is cast. While the crowns are being made, the cone is again covered with a former. The role of the gasket when installing the prosthesis on the implant is performed by the abutment. It is screwed on with a screw, and the head is isolated with a temporary filling before installing the “cap”. The crown itself is secured using glass ionomer cement. Read more about different types of implantation here.
PRINCIPLES FOR SECURITY OF PERSONAL DATA
3.1. The main task of ensuring the security of personal data during their processing in the Organization is to prevent unauthorized access to it by third parties, to prevent intentional software, hardware and other influences for the purpose of stealing personal data, destruction (destruction) or distortion of them during processing.
3.2. To ensure the security of personal data, the Organization is guided by the following principles:
- legality: protection of personal data is based on the provisions of regulatory legal acts and methodological documents of authorized state bodies in the field of processing and protection of personal data;
- systematic: PD processing in the Organization is carried out taking into account all interconnected, interacting and time-varying elements, conditions and factors that are significant for understanding and solving the problem of ensuring PD security;
- comprehensiveness: PD protection is built using the functionality of information technologies implemented in the Organization’s information systems and other systems and protection means available in the Organization;
- continuity: PD protection is ensured at all stages of their processing and in all modes of operation of PD processing systems, including during repair and routine maintenance;
- timeliness: measures to ensure an adequate level of PD security are taken before the start of their processing;
- continuity and continuity of improvement: modernization and expansion of measures and means of protecting personal data is carried out based on the results of an analysis of the practice of processing personal data in the Organization, taking into account the identification of new ways and means of implementing threats to the security of personal data, domestic and foreign experience in the field of information protection;
- personal responsibility: responsibility for ensuring the security of personal data rests with the Employees within the limits of their responsibilities related to the processing and protection of personal data;
- minimization of access rights: access to personal data is provided to Employees only to the extent necessary to perform their job duties;
- flexibility: ensuring the fulfillment of personal data protection functions when the characteristics of the functioning of the Organization’s personal data information systems, as well as the volume and composition of processed personal data change;
- specialization and professionalism: the implementation of measures to ensure the security of personal data is carried out by Employees who have the necessary qualifications and experience;
- efficiency of personnel selection procedures: the Organization’s personnel policy provides for careful selection of personnel and motivation of Employees, allowing to eliminate or minimize the possibility of them violating the security of personal data;
- observability and transparency: measures to ensure the security of personal data must be planned so that the results of their application are clearly observable (transparent) and can be assessed by those exercising control;
- continuity of monitoring and evaluation: procedures for continuous monitoring of the use of PD processing and protection systems are established, and the results of monitoring are regularly analyzed.
3.3. The Organization does not process PD that is incompatible with the purposes of its collection. Unless otherwise provided by federal law, upon completion of personal data processing in the Organization, including when the goals of their processing are achieved or the need to achieve these goals is no longer necessary, the personal data processed by the Organization will be destroyed or depersonalized.
3.4. When processing personal data, their accuracy, sufficiency, and, if necessary, relevance in relation to the purposes of processing are ensured. The organization takes the necessary measures to delete or clarify incomplete or inaccurate personal data.
What to do after installing a crown on a tooth
The time during which you cannot eat after a crown is installed depends on the type of cement. In addition, anesthesia is still in effect, and you can accidentally injure yourself. It is better to refrain from eating for 2-3 hours.
It is not recommended to load the side where the crown was installed - chew on the opposite side. Drinks and food with coloring pigments (red wine, berries, seasonings) should be kept to a minimum. It is recommended to avoid:
- sudden temperature changes (for example, drinking ice cream with coffee);
- solid food (bones, cartilage, nuts);
- sticky foods (taffy, some oriental sweets).
Hygiene requirements are standard: cleaning the mouth in the morning and evening. Superfloss, dental brush, and irrigator are recommended for bridges.
Main advantages
There are many advantages to using an artificial crown, some of which include:
- good aesthetic factors;
- long period of operation;
- affordable price;
- no need to sharpen teeth;
- biological compatibility of materials with dental tissues and gums.
A crown installed on the affected tooth will significantly extend its service life and functionality. Ceramic coating is resistant to pathogenic microorganisms, the result of which is caries.
Does it hurt to put a crown on a tooth?
The presence of a pain symptom during installation of a crown on a tooth depends on the tooth:
- on the pulpless one the pain is not felt. However, if you ask for additional anesthesia, they will give it;
- on “living” teeth, with the root preserved, there is an unpleasant sensation, pain is felt during grinding. Anesthesia solves the problem, but it is advisable to do a test to avoid an allergic reaction.
When installing dental crowns, when a temporary prosthesis is installed, the edge of the gum may be damaged and discomfort may be felt, but this is a normal process - no medications are required. If there is increased nervous excitability, the pain threshold is low - you can take sedatives and painkillers (be sure to discuss this issue with your dentist!).
Pros and cons of crowns
It is impossible to call the installation of crowns a uniquely positive procedure. It has a number of contraindications and disadvantages. But there are much more advantages from it, so it has not lost its relevance for decades.
Advantages
There are significantly more positive aspects of crown prosthetics than negative ones. The advantages of the procedure include:
- maintaining the health of the tooth when it is partially destroyed;
- restoration of chewing function of the jaws;
- protection against tooth decay with removed pulp;
- restoration of intelligible and clear speech;
- possibility of crown replacement;
- restoration of the aesthetic appearance of the smile.
A large number of advantages outweigh some of the disadvantages of the procedure. But they are still worth considering before deciding to install.
Flaws
Like any medical procedure, crown placement is not without its drawbacks. Its disadvantages:
- significant grinding of healthy tooth tissue;
- the procedure is not performed if the root is damaged;
- limited crown service life;
- the need for regular monitoring by a doctor.
Despite the number of shortcomings, dental crowns remain popular and in demand. This is an effective way to restore the integrity of your smile and jaw function without significant financial investment.
Possible complications after the procedure
Complications are rare after crown placement, but complications do occur. Most often this is a medical error or lack of professionalism. Therefore, the best prevention of complications is choosing a clinic with an excellent reputation. In addition, there are several diseases that do not depend on the doctor. They can be caused by medications, gastrointestinal diseases, and injuries.
Complications after crown installation
Prosthetic stomatitis (allergy)
Stomatitis, the cause of which is dentures, happens:
- allergic, this is a contact allergic inflammation, which often occurs after repeated prosthetics;
- toxic (occurs more often than allergic).
Prosthetic allergic stomatitis is a reaction to metal compounds and plastic. The more metal (a large number of bridges, crowns), the more likely an allergy. Moreover, this type can develop both immediately after installation and after 5-15 years of wearing crowns. Patients with gastrointestinal diseases and endocrine disorders are at risk. Typical complaints are swelling of the mucous membranes of the oral cavity and larynx, sometimes it is difficult to breathe, the tongue swells and does not fit in the mouth, but there are no ulcers familiar to ordinary stomatitis.
If a metal, metal-ceramic or metal-plastic crown is installed, a burning sensation of the tongue, drooling, and dry mouth are noted. If you are allergic to acrylates, granular bright red foci of inflammation appear on the mucous membrane of the palate, matching the shape and size of the prosthesis. In addition, skin reactions are noted - eczema, urticaria, dermatitis.
With toxic prosthetic stomatitis, the mucous membrane is damaged, and there is massive destruction of the epithelium of kidney, liver, intestinal cells, red blood cells, and nerve cells. Most often, poisoning is caused by stainless steel; if the crown (whole or base) is made of gold or a silver-palladium alloy, the disease occurs much less frequently.
This complication appears 1-7 days after installation. Characteristic symptoms of toxic denture stomatitis:
- burning tongue;
- drooling (hypersalivation);
- unpleasant feelings in the tongue, such as tingling, rawness (glossalgia);
- nervous disorders;
- gastrointestinal disorders.
Caries on supporting teeth
The ground teeth under the crown, if the nerve is removed, dry out over time. As soon as the seal is broken, bacteria and food particles penetrate under the denture and caries develops. That is why, even if part of the tooth and the root remain, it is better to build up the support than to remove the tooth along with the nerve.
Jaw trauma and hard food lead to a violation of the integrity of the crown and further development of caries underneath it. Development is promoted by poor oral care.
Galvanic syndrome
Saliva is a complex electrolyte, and the oral cavity is an electrochemical system in which:
- saliva (liquid phase), saturated with oxygen and carbon dioxide, acts as an electrolyte;
- teeth, dentures (solid phase) act as electrodes.
If there are metallic inclusions in the oral cavity that are not covered with ceramics (insulator), the potential of the electrode system increases sharply. There is a feeling of acidity and burning in the mouth. With a galvanic symptom, the functioning of the nervous system is disrupted, which leads to a general deterioration in the patient’s condition.
GENERAL PROVISIONS:
1.1.
This Policy regarding the processing of personal data (hereinafter referred to as the Policy) is drawn up in accordance with clause 2 of Art. 18.1 of Federal Law No. 152-FZ of July 27, 2006 “On Personal Data” as amended by Federal Law No. 16 of February 22, 2017, and is the fundamental internal regulatory document of the Limited Liability Company “SELLADENT” (hereinafter referred to as the Organization), defining key areas its activities in the field of processing and protection of personal data (hereinafter referred to as PD), the operator of which is the Organization. 1.2. The policy was developed in order to implement the requirements of the law in the field of processing and protection of personal data and is aimed at ensuring the protection of the rights and freedoms of an individual and citizen when processing his personal data in the Organization, including the protection of rights to privacy, personal, family and medical secrets.
1.3. The provisions of the Policy apply to relations for the processing and protection of PD received by the Organization both before and after approval of the Policy, except for cases where, for reasons of legal, organizational and other nature, the provisions of the Policy cannot be extended to relations for the processing and protection of PD received before its approval.
1.4. PD processing in the Organization is carried out in connection with the Organization’s performance of the functions provided for by its constituent documents and determined by:
- Federal Law of November 21, 2011 No. 323-FZ “On the fundamentals of protecting the health of citizens in the Russian Federation”;
- Federal Law No. 152-FZ of July 27, 2006 “On Personal Data”; Federal Law No. 16 dated February 22, 2017
- Decree of the Government of the Russian Federation of September 15, 2008 No. 687 “On approval of the Regulations on the specifics of processing personal data carried out without the use of automation tools”;
In addition, the processing of personal data in the Organization is carried out in the course of labor and other directly related relations in which the Organization acts as an employer (Chapter 14 of the Labor Code of the Russian Federation), in connection with the implementation by the Organization of its rights and obligations as a legal entity.
1.5. The organization has the right to make changes to this Policy. When changes are made, the date of the last update of the edition is indicated in the title of the Policy. The new version of the Policy comes into force from the moment it is posted on the website, unless otherwise provided by the new version of the Policy.
1.6. The current edition is stored at the location of the Organization at the address: Moscow, st. Novoryazanskaya 38, building 3, electronic version of the Policy - on the website at: https://www.al-bis.ru/about/confidential/
When should crowns be removed?
Crowns are removed if:
- they are worn out (stains appeared on metal ones, cracks and chips appeared on ceramics);
- loose fit;
- caries develops under the crown, especially deep ones.
The most common, simple, fast method is sawing, which is carried out with a special drill. The crown is not sawn completely: notches are made, then the crown is expanded from below and removed. If the tooth is not pulpless, this operation may be painful. The disadvantage is that the crown is damaged and cannot be restored.
To remove crowns, if they are installed on phosphate cement (or analogues), crown removers (for example, a Kopp apparatus) are also used. They are accompanied by removable hooks of various sizes, which are used to act on the edge of the prosthesis, displacing the crown, and then removed. The crown will remain intact, but will be scratched.
The Coronaflex device destroys cement using a shock wave. The crown remains intact under this influence and is reused. The most expensive method, the device is used mainly for “caps” made of zirconium dioxide.
Another method (not suitable for all materials): crumbling cement under the crown with ultrasound. A thin rod is inserted under the prosthesis, which vibrates and destroys the fastening.
Restoration of premolars and molars
When restoring chewing teeth, there are certain features: the structure must be resistant to any mechanical stress.
Most dentists recommend using the following methods for this:
- Implantation. When restoring the masticatory group, there are some disadvantages: the procedure is two-stage. The process takes a long time, but is popular. Bone grafting may be performed first.
- Clasp prosthesis. This is a base that looks like gum; crowns are subsequently installed on it. Recommended for use if there are no chewing teeth on both sides of the jaw. The main feature is that the load is distributed evenly; if other teeth have poor stability, this is important. But there are also disadvantages; if you want, you won’t be able to install ceramic crowns.
- Removable prosthesis. The option is considered one of the most budget-friendly. Nylon or acrylic dentures can be used.
Plastic crowns
As you can see, all recovery methods are different and have both disadvantages and advantages.
How much does it cost to install a crown on a tooth?
The final cost of prosthetics depends on the crown material, treatment plan, associated costs (radiovisiograph image, impression, anesthesia, etc.).
| Type of crown | Price for 1 tooth, rub. |
| Metal | From 4500 |
| Metal ceramics | From 9000 |
| Zirconium dioxide | From 17500 |
| Plastic | From 2000 |
| Metal-plastic | From2500 |
| Sitall | From 14000 |
| Ceramics | From 13000 |
Types by time of application
There are various artificial crowns and their types. Their classification largely depends on the time of application. In this case, temporary and permanent structures are distinguished. They are selected depending on the problem that needs to be solved. Temporary crowns are made to solve problems such as:
- change in bite height;
- protection of the soft part of the tooth;
- fixation of special devices.
Such products are installed for a short period of time, that is, until permanent structures are installed, and then they are removed. The choice of such products is quite wide and depends on the characteristics of the tooth, which has a certain location. Polyethylmethacrylic or polycarbonate products are suitable for the front teeth. For chewing teeth, crowns made of special medical alloys are used. Temporary structures are installed on a special fixing device and are easily removed when necessary.
Permanent crowns can be of several types, which vary in quality and cost. The materials used are mainly plastic, composites, and ceramics. For example, ceramic products are suitable for people prone to allergies. They differ in that they do not irritate the gums and look as natural as possible.
For the manufacture of metal structures, steel, cobalt, gold, and chrome are used. Such products are characterized by the fact that they combine aesthetic appeal, durability and affordable cost. To make your teeth look as natural as possible, it is best to choose gold alloys.
Zirconium dioxide crown
Zirconium dioxide crowns
– these are the most modern, ultra-strong and highly aesthetic crowns that are as similar as possible to natural tooth tissue. Today, zirconium dioxide is recognized as the best material for dental treatment. It has many advantages and virtually no disadvantages.
A zirconium tooth crown has the following advantages:
- Excellent aesthetic properties: shade, color, structure, light transmission;
- Maximum natural and beautiful appearance;
- Maximum restoration of tooth functions;
- Possibility to make for any tooth;
- Bioinertness and hypoallergenicity of the material;
- Very high strength and reliability;
- Tight fit and secure fixation;
- Durability of color and aesthetics over time;
- Can be used for metal allergies;
- Many positive reviews from patients and specialists;
- Absolutely safe for the oral cavity and the body as a whole;
- The fastest and most modern method of treatment;
- Longest service life and warranty.
The disadvantages of the products include high cost, complex manufacturing process and the need for special modern equipment.
Prosthetics
Treatment with zirconium dioxide crowns can be carried out in 1 or 2 visits to a specialist. Modern equipment and materials are used for prosthetics: a 3D scanner, an intraoral camera, a milling machine and special computer software. An examination of the oral cavity organs, radiographic examination, sanitation of the oral cavity, and professional hygiene are carried out.
The dentist prepares dental tissues for the crown using special burs. Next, the dentition is scanned and a model is created on a computer. The shape, color and all the features of the future crown are modeled on a computer using special programs. A specialist starts up a modern milling machine to make the crust. Milling and creation of an orthopedic structure from a zirconium dioxide blank takes place. The doctor tries on the finished crown and fixes it in the mouth.
After treatment, it is recommended to carry out professional hygiene and preventive examination by a specialist every 6 months. Proper hygienic care guarantees a long service life - 15 years or more.
How long does the procedure take?
The duration of the procedure depends on the type of dental crown and the wishes of the patient. Usually several visits to the dentist are required. During the first visit, the doctor will conduct a consultation and refer the patient for an x-ray. After this, impressions of the teeth will be made, and then dentures. The duration of one session depends on the complexity of the work and the number of crowns; on average, the patient has to spend 1-2 hours in the dental chair.
It is important to know. The durability of crowns largely depends on the quality of the dentist’s work. Therefore, choosing a clinic must be approached very responsibly.
How to take impressions correctly?
If the mucous membrane was damaged when grinding the native crown, the procedure for taking impressions should be postponed until it is restored.
- In some patients, the injured gum can give recession - move away from the neck of the tooth and expose its root.
- Due to the presence of blood, the materials used to obtain impressions may not clearly depict the formed ledge.
As a result, the edge of the manufactured and installed crown will stick out above the gum, which will significantly reduce the aesthetics of prosthetic treatment of the front teeth.
Manufacturing and installation
The technology for making stamped dentures is simple; all you need are consumables, tools and the professionalism of a dental technician. The prosthetic procedure includes a clinical and laboratory stage.
Clinical
- Diagnostics
- examination by a doctor, x-ray diagnostics, drawing up a treatment plan, choosing the type of prosthesis. - Preparation
- preparation of the tooth for a stamped crown to the thickness of the structure (
0.25-0.3 mm
), taking into account safety zones, determination of central occlusion. If the tooth is rotated around its axis, the most protruding areas are ground off to correct its position in the row. - Impressions
– taking impressions of both jaws, installing a provisional (temporary) crown made of polymerizing plastic. - Installation
– control fitting, fitting of the prosthesis, fixation with dental cement.
Laboratory
The laboratory stage of manufacturing a stamped crown includes:
- Plaster modeling
– a plaster blank (model) is created based on the impression.
It is modified - a small depression is formed in the gingival area (about 0.5 mm
). The plaster model is trimmed, given more accurate contours, preserving all anatomical details, and checked in an occluder. The anatomical features of the tooth surface are reproduced using modeling wax. - Making a metal stamp
- using a plaster stamp, a metal stamp is made by casting. For each dental unit, 2 stamps are made - for preliminary and final stamping of the orthopedic system. - Pre-stamping of crowns
- the technician selects a sleeve according to the diameter of the dental crown so that it fits onto the metal stamp with some effort. If there is no sleeve of a suitable size, then use a workpiece of the closest possible diameter, pulling it through a special apparatus. The sleeve is fired, cooled, placed on the first stamp, and tapped with a hammer to give it a preliminary anatomical shape. The stamp is driven into the sleeve until the imprint of the chewing surface or cutting edge appears. The preliminary crown is removed by melting the stamp, fired, and cooled. - Final stamping
- the preliminary crown is placed on the second stamp and tapped with a hammer to obtain the correct anatomical shape. The workpiece is placed in the apparatus and subjected to pressure of 3-5 tons. They tap it again with a hammer, cut it to the level of the gums, and send it to the orthopedist for fitting to the patient. - Finishing
– after fitting, the workpiece is again transferred to the laboratory, bleached in an acid solution, ground and polished to make the surface smooth and shiny. At the request of the patient, the prosthesis is covered with ceramic lining or spraying. The finished prosthesis is handed over to the orthopedic dentist.
If it is impossible to process a solid sleeve on a model, soldering technology is used. To do this, the cap sleeve is cut into 2 or 3 parts, each part is modeled with a hammer on a stamp, then all the elements are connected into a single structure by soldering. The tooth for a stamped crown is prepared minimally, since the thickness of the walls of the prosthesis does not exceed 0.2-0.3 mm
.