Removing a tooth is the last thing a dentist will suggest. Due to a number of subjective and objective reasons, it is impossible to maintain the dentition in ideal condition until old age.
Dental defects are the loss of one or more dental units, leading to a violation of the integrity of the dentition, deviation in the development of physiological occlusion, and an abnormal arrangement of individual teeth.
Reasons contributing to the development of dental defects
Dental defects arise due to:
- untimely treatment of caries;
- inflammatory processes in the oral cavity;
- presence of malocclusion;
- genetic conditioning;
- diseases leading to changes in metabolic processes;
- damage to the jaw apparatus;
- various neoplasms.
Classification of dentition defects
There are several types of classification. Dentists mainly use three of them:
- Kennedy classification:
- Group 1 - bilateral absence of chewing teeth;
- Group 2 - unilateral absence of a molar;
- Group 3 - unilateral absence of lateral teeth with preservation of distal support;
- Group 4 - defect of the anterior jaw.
- Beltman classification:
- Class 1 - the defect includes edentulous chewing teeth.
a) dentition with unilateral terminal defects;
b) dentition with bilateral terminal defects.
- Class 2 - there is one or more included defects (if the terminal units are present, there may be no teeth in other parts of the row).
a) the number of missing units does not exceed three;
b) the number of missing units is three or more.
- Classification according to the Gavrilov system:
- Group 1 - dentition with terminal one- and two-sided defects;
- Group 2 - dentition with anterior and lateral one- and two-sided defects;
- Group 3 - combined defects;
- Group 4 - single preserved dental units.
Prevention of wear of hard dental tissues
For the purpose of prevention, it is necessary to identify and eliminate risk factors that are important in the occurrence of tooth wear. These include the patient's use of highly abrasive hygiene products, frequent consumption of drinks and foods with low pH, eating disorders, bruxism, disorders of occlusal relationships, and somatic pathology.
Basic strategies for preventing wear of hard dental tissues, based on the main risk factors:
1. A balanced diet with minimizing the consumption of foods and drinks with low pH.
Careful assessment of dietary habits is important in assessing the erosive potential of a diet. The patient should be familiarized with a list of foods with low pH (salad dressings, vinegar, alcoholic beverages, carbonated soft drinks, herbal teas, fruit juices). The patient is advised to keep a food diary for at least 4 days, including weekends. Identification of consumption of foods and drinks with low pH in any combination more than 4 times [17] per day allows the patient to be classified as at risk of dental erosion.
2. Control of hygiene skills and informed choice of hygiene products.
Scientists assign the leading role in the erosive and abrasive wear of tooth tissue to mechanical factors: the active use of certain abrasive hygiene products, irrational brushing of teeth [18-21].
Patients at risk (gastrointestinal diseases, eating disorders, hazardous occupations, bruxism, etc.) should use toothpastes with a low degree of abrasiveness (RDA index = 30-50) and a soft toothbrush. It is not recommended to cleanse immediately after consuming fruits and drinks with low pH, vomiting, regurgitation or reflux.
To prevent erosion, at least 1 hour should pass between meals or drinks.
3. Strengthening hard tissues and normalizing saliva function. Strengthening hard tissues is possible due to fluorides and calcium phosphate technologies.
Scientists have recognized effective technologies for increasing the acid resistance of hard dental tissues using fluoride-containing preparations [22]. When exposed to erosion, there is no need for remineralization of the subsurface layer. The main thing is to strengthen the thin surface layer. Therefore, when treating erosions, high concentration fluoride applications are a more appropriate application. Fluoride gels provide good protection for eroded enamel from the abrasive action of a toothbrush.
The use of bicarbonate-containing toothpastes is one of the ways to introduce buffering agents into the oral cavity [23]. It is recommended to apply alkaline pastes or gels before bed to protect teeth from erosion due to reflux that occurs during sleep.
Adding calcium and phosphate to sour drinks can significantly reduce their erosive potential. Juices and carbonated drinks containing calcium and phosphates have appeared on sale.
Measures to increase the secretion of stimulated saliva, such as chewing sugar-free gum, are accordingly anti-erosive and support remineralization.
4. Referral to related specialists for timely detection and treatment of somatic pathology (endocrine pathology, hormonal disorders, gastrointestinal diseases, serious eating disorders: anorexia, bulimia, bruxism).
The appearance of tooth wear may be associated with endocrine pathology, disorders of hormonal and mineral homeostasis. Yu. M. Maksimovsky (1981) assigns an important role in the development of erosions to hyperfunction of the thyroid gland. Dental erosions in patients with thyrotoxicosis were detected twice as often as in persons with normal thyroid function; a direct connection was established between the intensity of dental damage and the duration of thyrotoxicosis {24}. In women, dental erosions are detected in a higher percentage of cases {25}. Examination of patients with non-carious lesions of teeth should be carried out jointly with a gynecologist and endocrinologist. The examination algorithm by related specialists includes hormonal indicators (estradiol, TSH, prolactin, cortisol).
If gastroesophageal reflux is suspected, patients need a referral to a physician or gastroenterologist. The dentist should be alerted to erosions on the oral surface of the chewing group of the teeth of the upper jaw and the patient’s specific complaints (sour taste in the mouth, halitosis, increased salivation, permanent cough, stomach pain, feeling of a “lump” in the throat, burning sensation, hoarseness, belching, heartburn) . Patients with a history of asymptomatic gastroesophageal reflux report wet spots on the pillow and a sour taste in the mouth after sleep.
Eating disorders include three main diagnoses [26]: anorexia, bulimia, and other unspecified eating disorders (a combination of several disorders). Anorexia is characterized by a conscious refusal to eat, a prolonged lack of appetite, and the disappearance of the basic instinct - hunger; bulimia - uncontrolled eating of large portions of food, followed by spontaneous vomiting.
Early detection of eating disorders is important for the outcome of the disease, secondary prevention, prevention of complications and reduction of harmful consequences in relation to the dental health and general somatic status of the patient. Patients with eating disorders often avoid medical professionals, and if they do, they hide the true origin of the problem. Therefore, knowledge of the manifestations of these disorders in the oral cavity is extremely important for the dentist.
Symptoms and consequences of dental defects
Dental defects appear:
- chewing function disorder;
- incorrect bite;
- articulation disorder;
- single displacement of teeth;
- violation of the integrity of the dentition;
- violation of the aesthetics of a smile.
Diagnosis of dental defects
The removal of one or more dental units requires consultation with a dentist and an orthodontist, especially when it comes to the anterior part of the dentition. Untimely correction of the defect does not have the best effect on the condition of adjacent teeth.
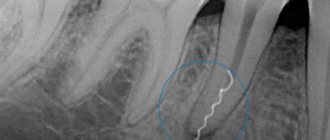
As a rule, a visual inspection is sufficient to determine how to correct the defect. In some cases, x-rays may be needed.
Destroyed crown part of the tooth
The crown is the visible part of the tooth, which consists of dentin and enamel. It bears the entire main load when chewing food, as well as the effects of an acidic environment, bacteria and a number of other factors. Despite its strength, the coronal part (like any bone tissue) is susceptible to destruction even if the rules of dental care are followed. This may occur gradually over time or be caused by injury and mechanical damage.
In any case, it is necessary to pay attention even to small chips, cracks in the enamel, and especially to incipient caries. Dentin does not have the ability to self-heal, so even minor defects that initially do not cause any discomfort subsequently lead to visible destruction. Suffice it to say that if you ignore the problem, then after just six months the coronal part may be half destroyed.
For information about prices and treatment times, call:
+7
or fill out the feedback form:
Causes of damage to the crown of the tooth
- Caries. The most common cause, which invariably leads not only to the destruction of the supragingival part of the tooth, but also to complications such as pulpitis. Caries can also be internal, which makes its timely detection much more difficult.
- Mechanical injuries. The second most common factor causing both minor and deep damage. Even constant brushing of teeth with hard brushes or the predominance of solid foods in the diet contribute to the gradual wear of the enamel. Visible damage causes impacts and strong pressure on the teeth, which can cause chips.
- Temperature effect. Constantly alternating cold and hot promotes the formation of cracks in the enamel, which over time can deepen and affect the dentin.
- Depulpation and secondary caries. Treatment of large carious cavities (especially with secondary intervention) leads to thinning of the coronal part. Removing the pulp (dental nerve) also causes it to decay more quickly.
- Poor nutrition. Insufficient supply of minerals, trace elements and vitamins, as well as metabolic disorders also gradually destroy the crown part of the tooth.
- Remineralization of enamel. Weakening and thinning of enamel occurs not only due to a lack of calcium or fluoride, but also due to hormonal imbalances or various diseases. This is why tooth decay often occurs during pregnancy and with diseases of the endocrine system or digestive organs.
How to treat a destroyed coronal part?
Treatment and recovery methods are determined depending on the degree of damage and its area.
– Installation of a seal . If tooth decay occupies about 20-30% of the area, then filling is performed with composite materials. First, the cavity is expanded and cleared of carious damage (if any), after which the coronal part is built up with composite materials. In some cases, it may be necessary to remove the pulp, even if the area is small - the carious process penetrates into the deeper layers and the nerve becomes inflamed.
– Restoration with a crown . With more serious damage, installing a filling often becomes ineffective - for example, if only one wall remains. In this case, a metal-ceramic crown is installed, which completely restores the coronal part with its chewing and aesthetic function. In case of severe damage, there is a need to strengthen the root. For this purpose, a pin is first installed, and then a crown is attached to it.
– Implantation . If not only the crown part is destroyed, but also the root is damaged, then the tooth will have to be removed. The most effective, reliable (and in some cases the only) method of restoration will be dental implantation. An implant is implanted into the root, onto which, after complete engraftment, a crown is installed. The capabilities of modern orthopedics make it possible to restore a tooth so that it is no different in shape, color and individual characteristics from the patient’s dentition.
Prevention of cracks in crown enamel
The best preventive measures are a balanced diet and careful treatment of your teeth. You should not eat hot and cold foods at the same time. This alternation leads to cracking of the enamel.
To maintain dental health, it is recommended to take dietary supplements. For example, a complex of calcium citrate and vitamin D. When brushing your teeth, you should give preference to medium-hard brushes and non-abrasive pastes. After eating, it is advisable to use dental floss.
To preserve your dental health, you need to undergo a preventive examination at the clinic twice a year and listen to the recommendations of dentists.
Treatment of cracks in tooth crowns
If the damage does not cause inconvenience and was discovered by chance, then a visit to the doctor is required. The defect should not be viewed as purely cosmetic.
Treatment depends on the type of chip and its severity. For minor damage, the doctor may suggest restoring the tooth crown with durable materials. In more serious cases, canal cleaning or tooth extraction will be required. In each specific option, the decision is made individually.
In case of micro-manifestations, remineralization is recommended, followed by surface coating with composites and varnish. It is possible to install veneers, and in case of significant damage, crowns.
Types of cracks
This phenomenon occurs frequently. Treatment depends on how the crown cracks—the direction of the split matters. In medical practice, there are several types of cracks.
Vertical crack
The vast majority are fixed on the front teeth. But it also happens on molars. It can stretch over the entire surface and, when neglected, affects the root. The integrity of the surface part is damaged, caries appears, quickly turning into pulpitis - such a crack opens the way to infection.
Horizontal crown crack
Statistics show: when the crown of a tooth is cracked like this, the destructive process is slower, and there is no accelerated danger to the pulp. If the crack is already large and there are prerequisites for chipping, then the tooth can be restored only by removing the damaged part and strengthening the tooth with a crown.
Oblique oblique
The pulp is often damaged. Treatment depends on the complexity of the specific situation. In an advanced state, only tooth extraction followed by implantation and prosthetics is possible.
Fracture of the tooth crown into pieces
A common option: separation - the crown of the tooth is cracked into 2 parts. The fragments put pressure on soft tissues and injure them. Food particles end up in the crack, causing pain. Treatment is urgently required; in case of serious pathologies, removal is practiced.
"Web"
Small cracks affect only the enamel of the tooth. At this stage, the treatment prognosis is favorable.
Damage to the masticatory tubercle
The pointed part of the tooth is injured. The result is a small chip. The pulp remains largely intact. It is possible to restore the tooth using modern filling materials or install a crown or veneer.
Methods for restoring a dental crown
The method of restoring the crown of a tooth is chosen by the dentist based on the size of the defect. Currently, reconstruction of the supragingival part is carried out in the following ways:
- Installation of a seal. The defect is filled layer by layer with composite material. The method is used for small damage (up to ⅓ volume). The advantages of the method are price, minimal time investment. Disadvantages - the filling changes color over time and stands out against the background of the enamel, and also requires replacement after 3 years.
- Installing a tab. For molar defects of more than ⅓ and less than ½ volume, ceramic inlays are used, which are made in a dental laboratory using an impression. The advantage of the method is efficiency and reliability (the inlay is much stronger than a filling and lasts up to 15 years). Disadvantages: complexity, price, need to wait for the product to be manufactured.
- Installation of veneers. The method is used for minor defects of teeth in the smile area (chips, cracks, stains). It involves removing enamel from the front surface of the tooth and fixing ceramic plates (veneers) with dental cement. The advantage of veneers is their multifunctionality; with their help, you can adjust the color, size, shape of units and at the same time eliminate minor defects. Disadvantages - restoration with veneers is irreversible and introduces some restrictions into the lifestyle.
- Prosthetics. Doctors recommend installing artificial crowns (made of ceramic, metal, zirconium, or combined materials) in case of more than half tooth decay, since other methods are not reliable enough. The advantages of the method are that it allows you to quickly restore the functions and aesthetics of a row. The downside is the price.
In case of loss of the crown and root parts, the integrity of the row can be restored using a removable prosthesis (butterfly or dental bridge). Complete restoration of the functions of the lost unit is possible through implantation (installation of a root prosthesis and an artificial crown).
To quickly restore the crown in the optimal way for you, sign up for a consultation with our specialists!
Author: Parnikel Vitaly Evgenievich orthopedic dentist, 1st qualification category
Treatment of wedge-shaped defect
Let's first consider traditional methods of treatment.
Applications of various preparations: varnishes, ointments, remineralizing solutions, etc.
The main advantage of this method is compliance with the most important Hippocratic principle: “Do no harm.” Indeed, this method of treatment will not harm the teeth. And it can bring benefits in the form of getting rid of hypersensitivity. True, after 10-15 visits, a single application is only enough for a few hours/minutes. It is impossible to eliminate the resulting defect by application, but you can get rid of the pain for some time.
Using toothpastes that reduce sensitivity (desensitivity)
This method includes all the advantages of the previous one, plus it has one more advantage - low cost. One tube of paste costs much less than 10-15 visits to the dentist, but the effect is approximately the same. Just as in the first case, it will not be possible to eliminate the defect itself and its further development. The maximum that can be achieved is the disappearance of pain in the necks of the teeth.
Filling with various materials
Glass ionomer, compomer, flowable or universal composites.
The most common treatment option for wedge-shaped defects. There are even more advantages: the pain disappears immediately after the first visit, and most importantly, the defect itself is eliminated and a fairly good aesthetic result is achieved. The trouble is that the cause of the disease cannot be eliminated by the most modern, best, most durable, most expensive filling.
This means that the mechanical load on the neck of the tooth will continue its negative impact. As a result, the fillings either fall out entirely, or (most often) remain in place, but at the same time they tear off one of their surfaces from the tooth, forming a gap into which food debris and bacteria become clogged. The photo clearly shows a dark strip between one surface of the filling and the tooth, the so-called “mourning border”.
It is undesirable to leave everything as it is - in addition to the progression of the wedge-shaped defect, you can now also get caries in this place. The old filling is removed, a new one is placed, and everything begins for the second round.
Installation of veneers
A veneer here means a ceramic veneer that covers the entire anterior and chewing (cutting edge of the front teeth) surfaces of the tooth.
This method is even better than the previous ones. In addition to superior aesthetics, it is sometimes possible to eliminate the cause (and therefore prevent recurrence of the disease for some teeth). But this will call into question the strength of the veneer itself. The maximum load will fall on it, and this structure is fragile to a certain extent. It may not be able to withstand the efforts from which the tooth’s own enamel has even been lost.
Therefore, veneers for wedge-shaped defects are most suitable for wealthy housewives and other citizens who have enough time and finances to regularly replace those that fail with new ones.
Manufacturing of artificial crowns (metal-ceramic or all-ceramic)
A radical, but very effective solution to the problem. Provided that the edge of the crown covers the wedge-shaped defect with a margin. But often this very reserve is not there - the defect is already located at the level of the gum, and grinding a tooth below the level of attachment of the gingival margin for a crown is strictly contraindicated. In addition, while protecting some teeth, crowns can put others at risk.
It turns out that even such generally reliable structures as crowns do not always solve the issue completely. A wedge-shaped defect can continue its destructive development on a tooth covered with an artificial crown and on neighboring teeth.
All of the above treatment options have one common drawback - they do not normalize the bite or eliminate the cause of the disease. Therefore, even if some of you, dear ladies and gentlemen, were helped by just toothpaste or a banal filling that has served faithfully for several decades, then consider yourself lucky. “Lucky” is such a capacious term in medicine, meaning that, despite inadequate treatment, a change in the living conditions of the body led to spontaneous self-healing.
In this case, destruction, mobility, installation of a large composite restoration or removal of the antagonist tooth will lead to the elimination of the etiological factor of the wedge-shaped defect. But a patient, much less a doctor, should hardly count on such dubious “luck.”
One of the most important tenets of medicine is: “Treatment must be predictable.” That is, to give a positive result in the maximum possible number of patients. In our opinion, it is not possible for a doctor who considers a wedge-shaped defect to be a “disease of unknown etiology” or who knows the cause, but for some reason ignores it, to achieve such a result.