General overview of the procedure
Gum coagulation in dentistry is a process during which diseased tissue is treated, cauterized, and also excised under ultra-high temperature. The procedure can be performed using different heating sources: heated instruments, electrocoagulators. Also, such an operation is often performed using a laser - it has the most gentle effect.
The description of the procedure sounds a little scary, but in fact this technique is completely safe for the patient’s health, as well as his psychological state. Do you agree that the absence of a scalpel (in the classical sense) and the need to carry out extensive intervention immediately puts you in a positive mood? In addition, the procedure is performed under local anesthesia, which means you will not feel any pain and will not have to be afraid of extremely high temperatures.
On a note! Thanks to the influence of special devices during cutting off damaged areas, the specialist performs the procedure with maximum accuracy and comfort for the patient. The soft tissues on which the intervention is performed are immediately cauterized using an instrument, so they do not bleed and remain sterile (they are disinfected), and also heal quickly during the rehabilitation period, which avoids complications and significantly reduces treatment time.
What is “hot” filling?
The correct name is the method of vertical condensation of hot gutta-percha. Long, difficult, not clear. Let's figure it out now!
Yes! “Hot” filling is only possible for root canals! There are no “hot” fillings (well, except maybe metal ones - although very few clinics work with them these days).
So, when filling the measles canal, the dentist’s main task is to fill the canal as tightly as possible with filling material. Not even the smallest gap should be allowed between the filling material and the wall of the root canal. If such a gap (empty space) is left, an infection will certainly begin to develop in it, which will ultimately lead to complications and the need to re-treat the tooth. Or even removal.
Today there are four main methods of filling root canals:
- one paste method;
- single pin method;
- method of lateral condensation of cold gutta-percha;
- method of vertical condensation of hot gutta-percha.
The first two methods, despite their fairly frequent use, cause quite a lot of complications, because cannot provide maximum obturation (filling) of the root canal with filling material. And if you really have to choose, then you have to choose between the methods of lateral (cold) or vertical (hot) condensation.
Read more about filling root canals
What is the difference between “cold” and “hot” filling?
With “cold” lateral condensation, the doctor inserts several gutta-percha pins of different diameters into the lumen of the root canal until the canal lumen is filled as densely as possible. Additional sealing is achieved through the preliminary (before the pins) introduction of a special paste into the canal - a sealer.
A gutta-percha pin is a thin column of a special plastic material (somewhat similar to rubber), which is inserted into the lumen of the root canal to seal it. Gutta-percha points come in different diameters. They should not be confused with titanium or fiberglass posts that are used as a basis for attaching a filling.
So, with “cold” filling, the lumen of the root canal is filled with several gutta-percha pins of different diameters until the entire canal is filled.
During “hot” filling, one thermoplastic pin, preheated in a special oven, is inserted into the lumen of the root canal. The diameter of the “hot” pin is selected so that it fills the entire lumen of the root canal. And, of course, the pins for cold and hot filling are different from each other and are not interchangeable!
Why is the gum most often cauterized?
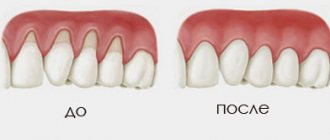
Most often, patients are recommended to apply electric shock to the affected areas due to hyperplasia or overgrowth of soft gum tissue, also called papillae. They fill the interdental spaces and are very sensitive to any impact. Their excessive enlargement and inflammation are caused by household injuries (occurring when using floss to remove plaque, toothpicks, brushes with hard bristles, or eating hard foods), dental diseases, poor oral hygiene, malocclusions, or hormonal disorders.
In the absence of proper treatment, the area of the interdental papillae increases, the soft tissues begin to become inflamed and bleed, causing pain and discomfort. In addition, the formation of such growths can cause problems with the correct pronunciation of sounds, impaired blood circulation in the gums, lack of adequate nutrition, and the appearance of complexes (overgrown mucous membrane can completely cover the crown part of the tooth, which looks extremely unaesthetic), so dentists recommend cauterizing them in a timely manner.
Stopping bleeding during dental restoration
November 7, 2013
Introduction
Traxodent paste
It would be great if the gums did not bleed, since blood entering the surgical field greatly complicates the restoration of teeth. The cause of bleeding gums during restoration operations is dental plaque or trauma. Plaque leads to gingivitis, caries or periodontitis. Trauma that results in bleeding may occur during surgery. The wedges exert lateral pressure on the periodontal papilla. The cavity sealing process uses metal or plastic matrices with sharp edges that can injure healthy or inflamed tissue. Dental burs are used to remove caries, excise inflamed tissue and widen the gingival sulcus. Retraction cords are placed to deflect or pull back the gum in an attempt to reach the edges of the cavity. All this leads to blood contamination of the restoration area, which in turn complicates procedures such as taking accurate impressions, preparing the dental cavity, prosthetics and cementing. This problem is typical for orthopedic dentistry.
Dental prosthetics and periodontal condition are interconnected. Poor dentures may have ridges and difficult-to-clean areas that allow plaque to accumulate. In adolescents and older adults, oral hygiene may be poor. Insufficient prevention of plaque formation leads to the need for dentures. In addition, the main contributing factor to dental prosthetics in patients in the following case studies is a diet high in highly refined carbohydrates (carbonated drinks) and lack of nutrients (refined foods).
Rice. 1 Blood got into the first impression, resulting in voids
In order to exclude the development of gingivitis or periodontal pathology, it is necessary to ensure an accurate marginal fit of the prosthesis. A good example is fixed orthopedic restoration. The fit of the prosthesis depends on the completeness of the impression. If the dental laboratory receives an impression that is incorrect due to blood contamination, problems with the prosthesis arise. Based on such impressions, stamps will be inaccurate due to the formation of voids and bubbles. (Picture 1). If a commercial dental laboratory produces a denture using an inaccurate die, the dentist will receive an inaccurate denture that will not fit the patient and will be rejected. Everyone will be disappointed - the patient, the doctor, and the dental laboratory. As a result, everyone loses income. The patient will need to take time off work, the doctor will need to provide additional chair time, and the dental laboratory will need to facilitate the entire process. When a problem occurs, people usually blame it on someone else. For the dentist this may seem like a personal failure, but in reality it is a systemic failure. If this system is not corrected, the dental office's main source of income will suffer. The main task is to understand how blood and gingival fluid enter the surgical field during restoration work, and what can be done to improve the control system.
The defective impression was made according to a standard procedure using a retraction cord soaked in a hemostatic solution and a one-step impression. The thread was placed on the inflamed tissue to treat subgingival caries. Treatment of subgingival caries required subgingival extension of the tooth core, which led to the need for subgingival preparation for a crown. Bleeding of the tissue is typical for such cases. The system used must control bleeding during the impression taking process.
Rice. 2 Traxodent paste is applied to the bleeding groove
To ensure the accuracy of the indirect technique, a new impression must be taken. You should wash the bleeding tissue and try to dry the wet area. A straight cannula is attached to the Traxodent syringe. In this case, the cannula was bent over the handle of the mirror at an angle of 90°. This facilitates positioning in posterior areas of the mouth where direct access is not possible. Traxodent paste should be applied over the bleeding tissue, slowly squeezing over the gingival sulcus along the edge of the preparation.
The paste can remain in the groove for 1-2 minutes (Figure 2), then it must be rinsed with a water/air gun. After washing and drying, no bleeding is observed, the gingival sulcus becomes dry. To obtain a one-stage impression, impression material of low and medium viscosity is used. Other types of impression material are used with no less success.
Fig. 3 The repeated impression, in which no blood has entered thanks to Traxodent paste, has no voids
Traxodent paste is a retraction system based on Hemodent paste. The paste contains aluminum chloride, which causes tissue retraction and contraction. Aluminum chloride promotes protein precipitation, contraction of blood vessels and removal of fluid from tissues. Aluminum chloride-based paste reduces the risk of postoperative inflammation. Aluminum chloride is the least irritating of the retraction medications. This drug, placed in the groove, does not cause noticeable gum recession. Pallor of the gums is the first sign of the paste's action. After this, the oozing blood turns brown and stops flowing. These two signs indicate hemostasis and a positive result of impression taking. (Figure 3).
Thanks to the methods used in this system, a flawless re-impression is obtained without the use of additional retraction cords. A re-impression using Traxodent paste is preferable because a small amount of impression material is left behind the preparation edge. This ensures that the edges of the plaster die are precisely processed in the laboratory, resulting in a precise fitting prosthesis.
Rotational curettage with Traxodent paste
Rice. 4 Blood and fluid in the gingival groove
Let's consider the case when the tooth has an inlay for building amalgam on pins. This tooth requires support from the entire crown. This tooth had a healthy groove and sufficient amount of attached gum. The entire crown requires a clasp to improve prognosis. Creating a clasp requires preparing the tooth to the bottom of the gingival sulcus. Rotary curettage was used to create a groove using a high-speed diamond bur to quickly remove epithelial tissue in the groove adjacent to the margin. Studies have shown that rotary curettage has little effect on gingival margin height if there is adequate gingival keratinization.
Rice. 5 Traxodent paste applied close to bleeding tissue
Rotational curettage is necessary to create 0.2 mm of thickness in the sulcus to maintain adequate thickness of the polyvinylsiloxane impression material. This thickness is required to create tensile strength and prevent breakage when removed from the oral cavity. Removal of the sulcus mucosa resulted in bleeding in the repair area (Figure 4).
Traditional methods would require the application of a retraction cord for 4 to 10 minutes to widen the groove. In this case, Traxodent paste was applied for 2 minutes to control the bleeding caused by rotary curettage (Figure 5). Additional deflection was mediated by the use of the Premier retraction cap (Figure 6). After rinsing with a water/air gun, only amalgam residues are retained. The groove is dry, hemostasis has been achieved (Figure 7).
|
|
Application of Traxodent paste in the aesthetic area
For aesthetic procedures on anterior teeth, creating a groove around the edge with a bur, floss or laser may not be desirable as it may detract from the appearance. Cosmetic restoration procedures are difficult because the preparation line is in close contact with the gum. If the root of the tooth is very dark, a dark line appears in the area of the neck of the tooth. Patients view this as a cosmetic defect.
Applying a thread can lead to ulceration or inflammation of the connective epithelium. The problem is that it is difficult to control the force of thread application. Other trauma, such as mechanical pressure or surgical damage, can cause unwanted migration of the gum line away from the margin. Traxodent paste is the least traumatic method of drying the field and causes slight displacement and retraction of the tissue.
Let's consider a clinical case. The patient is very concerned about the aesthetic outcome and does not like the dark contrasting color along the gum line. She had a cracked porcelain veneer that needed replacing. The tooth has already been prepared at the edge of the gingival sulcus. The tooth has already been prepared at the crest of the gingival sulcus, and the edges will remain in the same position (Figure 8). Due to accidental contact of the bur with the groove, some areas were damaged and began to bleed. Traxodent paste is applied to the groove and remains there for 1-2 minutes (Figure 9). The tooth is washed with an air-water jet and dried. The area is ready to receive an impression (Figure 10). A one-step impression using low to medium viscosity tray material will produce an accurate impression without bubbles or voids. When examined after 3 months, the margin remains stable and within the aesthetic zone (Figure 11).
|
|
|
|
Hemostasis with Traxodent paste for class II fillings
Rice. 12 The gums are accidentally damaged when drilling out caries
The risk of blood entering during the filling of class II cavities is as high as when installing a crown or bridge. This problem may mean longer procedures for the patient and changes in the dentist's chair schedule. Bleeding in the interproximal area is usually associated with caries (Figure 12). Bleeding begins from the inflamed interproximal gingival area if it is touched with a bur during removal of carious dentin.
Bleeding also occurs during isolation of a carious lesion when a ring, wedge or rubber gasket comes into contact with inflamed tissue (Figure 13). Traxodent paste is applied to the bleeding area located in the deepest part of the interproximal pocket (Figure 14). After 1-2 minutes, the paste is washed off with an air-water jet and hemostasis is confirmed. It is obvious that the entire surface of the cavity can be visualized, after which filling is carried out in the usual way.
|
|
Discussion
The value of these case reports is that they demonstrate a new hemostasis technology (Traxodent paste) that can solve common bleeding problems in the area of restorative treatment.
Thanks to its balanced fluidity, the paste can penetrate and remain in hard-to-reach areas of the groove. This balanced flow is important when treating the upper and lower dental arches, as the drug remains in the groove without getting into the laryngeal vestibule or throat. This is important for the patient, as the procedure becomes less unpleasant. Typically, hemostatic agents are strong astringents that create a dry, tight, and rough feeling in the mouth. This new technology is important for the dentist because it allows the drug to remain in direct contact and in its entirety in the gingival sulcus. There is no need to re-apply the drug due to dissolution by saliva or leakage. After application, the drug remains in place, even in contact with the tongue or cheek. Paste differs from liquid hemostatic agents in its ability to absorb liquids. Treatment areas adjacent to the mucous membrane of the alveolar processes of the jaw may become contaminated to deeper spaces. The physician should be aware of the problems that arise in such areas with insufficient adjacent keratinized tissue. As one of the warnings, we can mention the risk of leaching of the hemostatic drug into deep areas between tissues that are not intended for applying the product. The paste is not intended for the treatment of gingivitis, periodontitis and other diseases. The doctor should supervise the application of the paste to the dental treatment area. Traxodent paste is intended to be inserted onto the surface of the tissue, like a bandage, and not to be inserted into the submucosa.
Conclusion
Bleeding is a common problem that occurs during the dental restoration process. Common causes include plaque-induced erythema due to gingivitis, along with the use of instruments in the treatment area or the inadvertent use of instruments that create tears in the gingival tissue during restorative procedures. Any injury to the inflamed tissue leads to bleeding in the restoration area. Bleeding leads to deformation of the impressions, lack of adhesion of the filling and contamination of the cement.
Traxodent paste is a retraction system based on Hemodent paste, which contains aluminum chloride. Traxodent stops gum bleeding and causes temporary soft tissue contraction without further tissue damage.
Dean Eledge DDS, MD Associate Professor, AEGD
see also
September 13, 2013
Traxodent/Traksodent - material for hemostasis and gum retraction, Premier
Retraction system based on Hemodent® paste
March 21, 2012
PREMIER. Unconditional quality of dental materials
The American company Premier was founded in 1913. Soon it will be 100 years since Premier cherishes its traditions and values its reputation, so the company’s specialists carefully monitor the production process and always strive to improve the level of product delivery. UNIDENT presents the Premier line of dental materials, in which you can find materials that are indispensable for a dentist’s work.
October 30, 2011
Traxodent System: Predictive Management of Gingival Tissue
In modern dentistry, control of gingival fluid and gingival tissue is the primary criterion required for a successful clinical procedure. "Traxodent" is a unique system for high-level hemostatic processes. It is available in convenient syringes. Its paste-like consistency improves the retraction of gingival tissue, and 15% aluminum chloride, which is part of the paste, has very high hemostatic properties. Return to section
Therapy for hypertrophic gingivitis
The disease is one of the most common in dentistry - it occurs with equal frequency in both adults and children. It is characterized by the proliferation of soft interdental tissues, which, if left untreated, can overlap the crowns of the teeth. The appearance of pathology is provoked not only by poor oral hygiene and hormonal imbalance in the body, but also by chewing hard pieces of food that injure the interdental spaces, and improper use of personal hygiene items (threads to remove plaque, brushes, etc.).
In complex therapy (taking anti-inflammatory drugs, physiotherapy, gingivectomy) to treat the disease, dentists recommend using a method such as coagulation.
Coagulation of the gingival papilla
The procedure is quite in demand due to the careless attitude of most people towards their own health. Due to limited time or fear of dentists, many simply do not treat diseases of the gums and teeth, such as gingivitis, caries, etc.
As a result, the lesion site becomes overgrown with pathological gum tissue. This disease requires medical intervention, namely coagulation of the gingival papilla.
Inflamed gingival papilla
Cauterization is performed under local anesthesia and during the procedure the patient feels only mild discomfort. Thanks to the use of an electrocoagulator, healthy tissues are not affected by the instrument.
Oral care after the procedure
The postoperative period is quite unpleasant and painful, since, in essence, a part of the living mucous tissue, albeit of a pathological nature, was surgically removed. The pain syndrome will accompany the patient for two days after the operation, after which it will gradually recede. To alleviate the condition, the doctor may prescribe analgesics.
Rinsing with herbal decoctions or chewing propolis will help relieve pain.
The recovery period after surgery takes on average from 2 to 10 weeks . This is exactly how much tissue needs to fully regenerate. During this time, the patient must regularly visit the attending physician’s office to monitor the condition.
The doctor may prescribe rinsing with an antiseptic solution of Chlorhexidine or Furacilin and the use of anti-inflammatory ointments. It is very important to prevent infection from entering the treated tissue areas.
Furacilin
Depending on the nature of the disease, the doctor may prescribe antibiotic medications in order to completely destroy the pathogenic microflora and prevent re-complications.
Other situations when the procedure is performed
Such a modern treatment method as coagulation is often used in dentistry for the following purposes:
- removal of formations on the mucous membrane: malignant and benign,
- removal of any granulation tissue,
- correction and plastic surgery of gums to give an aesthetic smile,
- treatment of periodontitis and periodontal disease (only in complex therapy): in particular, the procedure can be carried out to cauterize and treat inflamed gingival papillae that have grown during the course of the disease. And also for removing granulations and pathological tissues from periodontal pockets - at the end of the procedure, the periodontal pockets remain completely sterile, the tissues fit tightly to the tooth, which prevents plaque, bacteria and food particles from getting inside,
- cauterization of inflamed gingival papillae: pathology can occur not only against the background of periodontal tissue diseases, but also due to trauma to the mucous membrane, malocclusion, hormonal disorders in the body, incorrectly performed dental treatment, chipped fillings and the presence of uncomfortable prosthetic structures,
- removal of papillomas, fibroids: they may look harmless, but sometimes they grow greatly, causing inconvenience, and become dangerous to health.
Who should not undergo the procedure?
Despite the fact that the described technique has a number of advantages (in comparison with traditional methods of surgical interventions), there are also some contraindications to the operation. Coagulation is not performed if the following problems have been diagnosed:
- intolerance to low-frequency electric currents: in this case, it is permissible to use only a laser,
- exacerbated infectious diseases,
- disorders of the cardiovascular system: there is a high probability of increased blood pressure,
- disruption of the hemostasis system: the risk of bleeding increases,
- chronic diseases: for example, diabetes.
Also, the use of “hot” instruments is unacceptable during the active change from primary to permanent occlusion in children, which occurs between the ages of 6-8 and 12 years.
Important! If the patient has the above conditions, the operation should be performed only under the supervision of a highly qualified specialist, and also provided that the likely harm from the development of the disease outweighs the risks of complications after coagulation.
Coagulation methods
There are several options for treating the affected mucosa. Depending on which device is used, the following methods are distinguished:
- cauterization with a metal instrument with a hot tip: the instrument is considered obsolete and is rarely used nowadays - the procedure using it is quite traumatic, and the subsequent rehabilitation period is quite long,
- excision with an electrocoagulator: here, with the help of a device, electrical energy is converted into thermal energy. High-frequency alternating electric currents supplied through the tool “dry” and destroy damaged areas,
- treatment with a laser device: damaged tissues are “burned out” with a beam of intense light.
Coagulation techniques and its types
Removal of inflamed tissue can be done using different techniques. Each of them differs in the way the current is supplied. There are two types of coagulation. Let's look at each of them in more detail.
Monopolar method and its features
The doctor uses an instrument that looks like a scalpel. But the effect on tissue is carried out not mechanically, but with the help of an electrode built into the scalpel handle, through which current is passed. In this case, electrical impulses (weak charges of safe alternating voltage) pass through the entire human body, and the safety of the process is ensured by a special return plate with which the tool is equipped. The presence of this element is mandatory, because it is responsible for the process of closing the electrical circuit.
The method is effective when performing coagulation to remove large tumors.
On a note! If cutting is performed with a faulty device or by an unqualified specialist, consequences such as injury and burns to the mucous membrane may occur during the procedure. The method is considered quite outdated these days, so doctors rarely resort to it.
Bipolar method and its features
The main difference between this method of coagulation is that the current passes only through the affected areas of the tissue (the doctor acts on them pointwise), so a return plate is not needed for its implementation. The operation is performed with an instrument with a forked tip, which grips and clamps the gum so that the electrical circuit is closed directly in the area of the procedure.
Types of coagulation (cauterization) of gums
Monopolar technology
A special return plate is placed on the patient’s body, which is responsible for closing the electrical circuit. A weak electrical impulse is passed through the patient's entire body and through the surgical instrument. With this procedure, you can get rid of even large neoplasms and tumors located in the deep layers of tissue. Due to its effectiveness, this method is used more often than others.
Bipolar technology
An electrical discharge is passed locally, only through the part of the body in which the tumor or inflammation is located. Therefore, the end plate is not used. This method is effective for the treatment of mild dental diseases.
The gum cauterization method is widely used in dental practice and shows good results in the treatment of periodontal diseases.
Before performing the operation, the doctor examines the patient’s oral cavity for injuries to the mucous tissues, since their presence can cause complications.
Bipolar gum coagulation technology
Upon completion of the operation, the patient is given a list of recommendations and a prescription for medications. For each patient, recommendations are made individually, depending on the disease and its severity.
How to prepare for the procedure
There is no need for special preparation before coagulation, but you should do the following:
- visit different specialists: before the procedure, if necessary, the doctor may refer you for a consultation with other specialized specialists (infectious disease specialist, oncologist, periodontist),
- Avoid drinking alcohol several days before the procedure, as well as on the day of coagulation: it negatively affects blood clotting and the effect of medications and anesthetics used during the procedure,
- have a snack before the procedure: the snack should not be heavy, but you should not completely refuse food, because After the operation, you will not be able to eat for at least another 1-2 hours.
How is the procedure performed?
The operation is performed only by an experienced dental surgeon. First, the doctor will sanitize the oral cavity and administer anesthesia (in the case of using a laser, it is often possible to confine oneself to local “freezing” in the form of gels and sprays, since the procedure causes virtually no pain to the patient). Next, the specialist works with an instrument designed for coagulation and performs the necessary manipulations.
Important! The patient should relax in the dentist's chair and not make sudden movements. Otherwise, the hand of even the most experienced specialist may tremble, and the instrument will damage healthy areas.
The duration of the operation directly depends on the degree of complexity of the actions performed, but on average coagulation takes no more than 20 minutes.
When removing a dental nerve, the following methods are used:
- vital extirpation, which involves complete removal of the pulp from a patient under local anesthesia, - devital amputation, in which partial mummification of the nerve is performed using a special drug, - diathermy (diathermocoagulation), during which the pulp is killed using an electric discharge, after which the doctor removes the non-viable nerve.
Vital extirpation
This technique allows the patient to get rid of the diseased nerve in one visit to the dental office. The use of vital extirpation is possible for acute or chronic pulpitis in a tooth with well-passable canals. Depulpation by vital extirpation occurs in 10 stages, during which antiseptic treatment of adjacent teeth is performed, administration of an anesthetic, cleaning of the diseased tooth from caries, opening of the pulp and amputation of the nerve, after which the tooth is filled. The entire procedure takes no more than 2 hours, but requires careful preliminary preparation and diagnosis of the tooth.
Devital amputation
Devital amputation is practically not used in modern medicine, since it is associated with multiple complications and the occurrence of necrotic phenomena in the nerves located in close proximity to the pulp removed by this method.
Diathermocoagulation
The essence of diathermocoagulation is to insert a microscopic electrode into the pulp cavity and apply a small current charge, which kills the nerve and cauterizes the resulting wound. Diathermocoagulation requires minimal doctor intervention in the jaw bone, so the depulpation procedure is almost bloodless. Occasionally, bleeding occurs when a nerve is removed from large molars.
After tooth nerve removal, many patients will experience pain for several days when closing their jaws or when hot or cold food enters the mouth. The pain is relieved with analgesics and does not require additional treatment.
Thanks to qualified treatment, a pulpless tooth can last for several years, especially if it was subsequently covered with a crown.
Advantages of the method
In comparison with the long-familiar, classical methods of surgical interventions, coagulation allows you to gently and painlessly target pathological areas of tissue, as well as destroy pathogenic bacteria. In addition, the gums do not bleed after coagulation, heal faster and look attractive. Therefore, you should not delay your visit to the doctor for fear of unpleasant sensations. Timely assistance will be the key to the health of your oral cavity and the beauty of your smile.
How does the procedure work?
The operation is performed by a dental surgeon. Since the procedure is practically painless, it is performed under local anesthesia, which uses an anesthetic gel.
While sitting in the dental chair, the patient should try to relax as much as possible and not move . Due to sudden movements, the instrument in the hands of a specialist can shake and damage healthy tissue.
Using a laser beam, the doctor excises the inflamed areas of tissue or completely removes the tumor. In total, this type of operation takes a quarter of an hour. It may take more or less time depending on the patient's specific problem.
The main thing for the patient is not to move
For several hours after the operation, you should refrain from eating food so as not to damage the tissues that have become especially sensitive after the procedure and not to cause an infection. It is necessary to take special care to keep your mouth clean and rinse after every meal. Outside the home, you can chew gum or use dental floss.
To speed up regeneration and relieve discomfort, you can rinse your mouth with decoctions of medicinal herbs ( chamomile , oak bark , calendula , etc.).
In order to make sure that the operation will be successful and will not cause any complications, the dental surgeon can refer the patient to an oncologist, infectious disease specialist and periodontist for additional examination and health monitoring.
What complications may arise after surgery?
Many patients note that their gums hurt in the first few days after coagulation. This phenomenon is considered a completely natural consequence of the intervention. To reduce discomfort, you can take painkillers that you usually use and keep in your medicine cabinet.
If the pain does not disappear after some time, and additional alarming symptoms appear (inflammation and redness of the mucous membrane, the appearance of bad breath, discharge of pus), then be sure to visit a doctor. The specialist will tell you what to do to make the gums suppurate go away: for these purposes, antibiotics that destroy pathogenic microflora and treatment of the mucous membrane with antiseptics are most often prescribed.