The biomechanics of the lower jaw is considered from the point of view of the functional purpose of the dental system (speech, chewing, swallowing). Movements of the lower jaw are realized as a result of the interaction of the temporomandibular joint (TMJ), teeth and masticatory muscles.
This interaction is coordinated and controlled by the central nervous system. Voluntary and reflex movements are regulated by the neuromuscular system; they are carried out sequentially.
For example, the initial movements—biting food and placing it in the oral cavity—are voluntary. Chewing and swallowing are then carried out unconsciously.
Everything is not as simple as it seems
Directions of movements of the lower jaw
Forward, down, up, sideways
Movements of the lower jaw are possible in three directions, their list includes:
- vertical;
- sagittal;
- transverse.
Any movements in the lower jaw are realized under the condition of simultaneous sliding and rotation of its heads.
The distal fixed position of the lower jaw relative to the upper jaw is ensured by the TMJ. This joint also creates guide planes for forward, downward, and sideways movement. If there is no contact between the teeth, the direction of movement of the lower jaw is carried out thanks to the articulating articular surfaces and proprioceptive neuromuscular mechanisms.
The stability of the vertical and distal interaction between the lower and upper jaws is ensured by the intercuspal contact of the antagonist teeth. In addition, thanks to the tubercles of the teeth, guiding planes are formed for the movement of the lower jaw forward and to the sides.
During the movement of the lower jaw, when the teeth are in contact, the direction of movement is determined by the chewing surfaces of the teeth, and the joints perform a passive function.
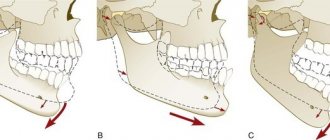
Vertical movements
Movements when opening the mouth
Vertical movements that characterize the process of opening the oral cavity can be carried out under the condition of active bilateral contraction of the muscles that go from the lower jaw to the hyoid bone. In addition, the heaviness of the jaw itself also plays a role.
Mouth opening has three phases:
- insignificant;
- significant;
- maximum.
The amplitude of the vertical movement of the jaw is 4-5 cm. In the process of closing the oral cavity, the lifting of the jaw is achieved due to the simultaneous contraction of muscle structures.
In the TMJ, the heads of the lower jaw rotate together with the disc around its axis, then down and forward along the slope of the tubercles to the apexes during the opening of the oral cavity and in the opposite direction during the closing process.
Sagittal movements
They provide forward movement of the lower jaw. In this case, a complex of movements is carried out in the sagittal plane within the boundaries of movement of the interincisal point.
The jaw moves forward due to bilateral contraction of the lateral and medial pterygoid muscles, and partially the temporal muscles.
The movement of the head is divided into two phases:
- Sliding of the disc together with the head along the surface of the joint tubercle.
- Attachment of the articulated movement of the head around its transverse axis.
The sagittal articular path is the distance that the head of the jaw travels during forward movement. Its average size is from 7 to 10 mm.
Sagittal path angle
The angle of the sagittal articular path is the angle formed when the occlusal plane intersects the line of the sagittal path. It depends on the severity of the joint tubercle and the tubercles of the lateral teeth. The average angle is 33°.
The Spee curve (sagittal occlusal) runs from the upper third of the distal slope of the mandibular canine to the distal buccal tubercle of the extreme lower molar.
In the process of protrusion of the lower jaw, due to the presence of the Spee curve, interdental contacts arise, which ensure the harmony of occlusal relationships between the rows of teeth. Thanks to the sagittal curve, the unevenness of the occlusal surfaces is compensated, because of this it is also called compensatory.
The mechanism of forward movement of the jaw can be described as follows: during the movement, the head of the condylar process tends forward and down along the slope of the tubercle of the joint, the teeth of the lower jaw also tend forward and down. But when encountering the complexity of the relief of the occlusal surface of the teeth of the upper jaw, the teeth of the lower side form continuous contact with them until the dentition is separated due to the height of the central incisors.
During the process of sagittal movement, the central incisors located below will slide along the palatal surface of the incisors located above, that is, they pass the sagittal incisal path. The angle between the occlusal plane and the vector of the incisal path can vary, but its average value is from 40 to 50°.
That is, ensuring the preservation of tooth contacts in the process of jaw extension occurs due to the harmonious interaction between the articular and incisive paths and the tubercles of the chewing teeth.
Very important! If, in the manufacture of prostheses, both removable and fixed, the curvature of the compensatory curve is not taken into account, then overload of the articular discs is provoked. This inevitably leads to TMJ pathology.
Transversal movements
Transversal, or lateral movements are produced due to the predominantly unilateral contraction of the lateral pterygoid muscle. During movement of the jaw to the right side, contraction of the left lateral pterygoid muscle is observed, and vice versa. The jaw head on the displacement side rotates around a vertical axis.
On the balancing side (the side of muscle contraction), the head of the lower jaw slides along the articular surface of the tubercle along the articular surface of the tubercle forward, down and slightly inward, that is, it makes a lateral articular path. The angle of the transversal articular path (Bennett's angle) is formed between the lines of the lateral and sagittal articular path. Its average value is approximately 17o.
Bennett Corner (17) and Gothic Corner (110)
Lateral movements are characterized by some changes in the position of the teeth. The intersection of the curved transversal displacements of the anterior teeth at the interincisal point occurs at an obtuse angle. This is the angle of the transversal incisal path, which is otherwise called Gothic. Its average value is from 100 to 110o. It characterizes the span of the incisors.
Lateral movement to the left
On the working side, the lateral teeth are located with the same tubercles relative to each other, and on the balancing side they are in an open state. The transversal occlusal curve (Wilson) connects the buccal and lingual cusps of the chewing teeth on one side with the same ones on the other side. The radius of curvature of the Wilson curve is 95 mm.
It is important to consider the types of opening of the dentition:
- Canine guidance . When performing lateral movements of the lower jaw, the condylar process on the balancing side moves forward, down and inward. At the same time, the plane of inclination of the jaw changes. The opening of the dentition is observed only when the fangs come into contact.
- Canine-premolar guidance . At the moment of opening the molars of the working side, the canines and premolars come into contact.
Note! In the process of making fixed dentures, it is important to find out the type of release characteristic of a particular patient.
The type of opening is determined based on the height of the fangs and the opposite side. If this is not possible, a prosthesis with a canine-premolar type of guidance should be made.
This prevents overloading of the articular discs and periodontal tissues. Compliance with the radius of curvature of the Wilson curve helps prevent supercontacts of the chewing teeth when making lateral movements of the lower jaw.
Midpoint displacement trajectories
The central relationship of the jaws is the starting point of all movements carried out by the lower jaw. It is distinguished by the uppermost localization of the heads of the joints and the tubercular contact of the lateral teeth.
Afterwards, the jaw moves to a more stable position, in which maximum fissure-tubercle contact is possible. The sliding of teeth within 1 mm from the localization of the centric relation to the central occlusion is directed forward and upward in the sagittal plane. This is referred to as “center sliding.”
Important! The considered data is used in the process of programming the articular mechanisms of devices that simulate the movements of the lower jaw.
Hanau Five: the path to balanced occlusion
Balanced occlusion ensures proper stability and retention of complete dentures.
The basic concept of balanced occlusion is to optimize occlusal contacts not only in the state of centric occlusion, but also in the range of motion of the mandible. Achieving such a functional relationship in the structure of the occlusal scheme of complete removable dentures is ensured through the interaction of five main factors, called the Hanau Five in honor of Rudolf Hanau: articular guide (AG), incisal guide (RN), occlusal plane orientation (OP), compensating curve (CC) ) and cusp inclination (NB) (photo 1). The articular guide is the angle formed by the movement of the articular head along the articular tubercle in relation to the Frankfort horizontal line. The articular guide is usually registered when the mandible is advanced approximately 6 mm into a state of protrusion, after which it is transferred to the articulator to account for the articular elements during positioning of the prosthesis. The incisal guide represents the relationship between the anterior teeth of the upper and lower jaws. The specificity of this ratio may vary depending on the level of vertical and horizontal overlap, and is recorded during the fitting of wax analogues of dentures in the patient’s mouth.
Photo 1. Hanau Five: articular guide (black dotted line), incisal guide (red continuous line), occlusal plane orientation (blue continuous line), compensating curve (red dotted line), cuspal inclination.
To create a more aesthetic profile, sometimes it is necessary to slightly increase the level of vertical overlap to better visualize the incisors and achieve maximum imitation of the natural appearance of orthopedic structures. However, too large an increase in the incisal guide parameter can affect the activity of the masticatory muscles, which, in turn, can cause restrictions in the movements of the lower jaw. The orientation of the occlusal plane is an imaginary plane in relation to the height of the crowns of the anterior and posterior teeth. The OOP is usually aligned along the line from the wing of the nose to the earlobe, along the intermaxillary relationship of the bone ridge, the retromolar mandibular space, the lateral edge of the tongue and the edge of the closure of the upper and lower lips. This plane may be parallel to the inner surface of the prosthesis, but it may deviate from it in a fairly wide range depending on the inclination of the bone crest. Ideal conditions provide a relatively flat surface of the bone crest onto which the inner surface of the prosthesis can be fitted almost completely parallel.
On the other hand, with protrusion of the articular direction, a discrepancy between the OOP and the ridge plane may develop. During protrusion, a space is formed between the upper and lower distal teeth, the presence of which is called the Christensen phenomenon. The dental sets available on the market are characterized by variable morphology, depending on which different NB can be formed. In general, depending on the morphology of the cusps, artificial teeth are classified into anatomical, non-anatomical and semi-anatomical. It is logical that anatomical teeth are characterized by higher NB parameters. However, the level of this may change when teeth are installed along the compensating curve (CC) with the actual formation of OOP. For example, artificial teeth with a 30-degree orientation may exhibit a 20- or 40-degree level of NB when positioned on a 10-degree curve to reference the OOP. In this article, we will describe a formula for a more objective assessment of balanced occlusion using the principles of the Hanau Five, and also discuss its limitations when analyzing individual mandibular movements. To search for relevant publications on this topic, we analyzed the MEDLINE/PubMed database using keywords (Hanau five, articular guide, incisal guide, occlusal plane, compensation curve, cuspal inclination) published in English up to 2022.
Articulation in central (centric) ratio
The maxillary and mandibular teeth are positioned in complete dentures to maintain the proper height of the lower third of the face while being in relation to the central (which is essentially centric) position of the temporomandibular joint. When the teeth in the denture structure are in occlusion, the articular head should be in the most stable position relative to the articular tubercle (photo 2-3). This central position of the joint should also be in harmony with the state of the neuromuscular complex of the dentofacial apparatus. It is this position, which is the most reproducible and most recorded, that is used as a reference position in the rehabilitation of edentulous patients using complete removable dentures.
Photo 2. Distal teeth are in a state of occlusion when the joint is positioned in centric relation: right view.
Photo 3. Distal teeth are in a state of occlusion with the joint positioned in centric relation: left view.
The occlusal morphology of artificial teeth must be characterized by some kind of “flushing” design to ensure proper masticatory function. Artificial teeth are positioned to optimize the direction of masticatory forces during occlusal function while providing adequate height to the lower third of the face. The distal teeth are positioned to ensure adequate jaw stop in the centric relation position, while the anterior teeth should not be in occlusal contact. The anatomical shape of the teeth provides the opportunity for their occlusal closure in the tubercle-fissure contact, but when positioning the upper jaw model along the face arch, so-called occlusal barriers or interference can sometimes develop, which limit the ability to perform normal functions. According to Weinberg, occlusal interference can be minimized when the arbitrary transverse horizontal axis is within a 5 mm radius of the true hinge axis. However, occlusal interference may be more significant if the vertical parameter of occlusion on the articulator is incorrectly determined. Due to the significant proximity of the transversal horizontal axis, distal teeth are usually more “sensitive” to the development of occlusal interference compared to the anterior ones. The positioning of jaw models in the articulator should be carried out taking into account the movement of the lower jaw during the functions of closing and opening the mouth. The vertical articular axis must be long enough to position the OOP as a landmark for the articular axis. When installing models into an articulator with a short articular axis, the closing arc of the lower jaw model will be steeper than the closing arc of the lower jaw itself. Thus, in the area of the distal teeth, deflective occlusal contact on the cusps may occur, resulting in the appearance of an open bite in the anterior regions of the jaws. It is also necessary to remember that the central relation represents a whole set of positions, and not a specific point. When the jaw moves, the condyle leaves its resting state and begins to move along the medial edge of the glenoid fossa as the jaw moves. In addition, we should not forget that in the cycle of movements of the lower jaw there is also the concept of lateral shift in the range of up to 1 mm, which develops in the terminal stage of the motor cycle.
Articulation in a state of protrusion
As the mandible moves forward, the distal teeth become separated. When the articular and incisal guides are 0 degrees, the Christensen phenomenon simply does not develop. Also, the interocclusal space is not formed when the occlusal plane is flat, parallel to the Frankfurt horizontal. According to previous studies, the average articular guide value in edentulous patients is 36 degrees, ranging from 10 to 62 degrees. The maximum individual differences in the articular guide on the left and right sides of the TMJ are about 25 degrees. Symmetrical HF on both sides of the TMJ were noted in only 12.5% of the examined patients, while differences between the sides of the TMJ greater than 10 degrees were noted in about 21.4% of patients.
Disocclusion of distal teeth also does not develop in cases of inclined orientation of the occlusal plane, or in cases of correction of the compensation curve in order to raise the level of the occlusal plane in the area of the distal teeth (photo 4-5). Closure of the interocclusal space (Christensen phenomenon) can be caused by the formed morphology of the cusps of the distal teeth, rising above the level of the occlusal plane. Occlusal balance is maintained by angulation of the distal teeth, which is determined by the inclination of the occlusal plane, the compensation curve and cusps, and a combination of these parameters. The larger the articular guide, the greater the inclination of the occlusal plane, compensation curve and cusps must be to achieve a state of balanced occlusion during protrusion.
Photo 4. Balanced articulation in protrusion: right view.
Photo 5. Balanced articulation in protrusion: left view.
The articulator must be equipped with adjustable elements to adapt and program the articular component. In this case, the elements corresponding to the right and left sides of the TMJ must be independent in order to correspond to the asymmetrical path of the articular head on the right and left sides of the dentofacial apparatus. The path of the articular head is a nonlinear trajectory due to the arcuate convexity of the inclination of the articular tubercle. Because of this, the value of the composite guide may be ambiguous when programming joint elements in the articulator. The graphical registration method makes it possible to verify the entire trajectory of joint movements and restore it by correcting the joint guide. However, in truth, in most commercially available articulators, the function of reproducing a graphically recorded articular path remains limited or impossible. It is necessary to understand that the articular path in no way depends on the interincisal relationship of the anterior teeth. The size of the articular guide remains unchanged even when the pH value changes in order to correct phonetic or aesthetic parameters. At the same time, the movements of the lower jaw themselves may change somewhat with changes in pH. As the pH (sharper ratio) increases to meet the patient's needs, the occlusal plane orientation, compensation curve, and cuspal inclination also increase. According to Svenson's formula, the ratio of the slope of OOP, CC and NB is described as follows:
NB = RN + d (SN-RN), where d is the fraction of the distance from the point of the cutting edge to each cusp (photo 6).
Photo 6. Schematic representation of the parameter “d” as a fraction of the distance from the cutting point to the cusp.
According to this formula, tooth location (d) is a significant factor in reproducing the proper NB angle. The more anterior the tooth is, the lower the d value. When the PH parameter is greater than SN, premolars will have a higher BN value than molars. However, the last molar will display the greatest BN value in conditions where PH is less than SN.
Articulation in lateral excursion
The working articular head rotates along the vertical axis of the condyle, while the balancing head descends along the articular tubercle. The occlusal morphology of the distal teeth is independent of the rotational movements of the working articular head, but at the same time, disocclusion develops on the balancing side due to the downward movement of the condyle. To maintain balance in accordance with the asymmetric rotational movement of the mandible, it is necessary to ensure the appropriate level of inclination of the main occlusal components. The working inclination (the sum of the inclination of the orientation of the occlusal plane, the compensation curve and the cusps) depends on the pH value. At a pH value of 0 degrees, the working slope is a flat plane. As the inclination increases, the ratio of the incisors of the upper and lower jaw becomes more acute, however, this ratio is not directly proportional due to the individual specificity of the rotational movements of the articular head on the working side, because the condyle does not demonstrate strictly rotational movement. Its vertical axis shifts in the lateral direction with additional movements forward, backward, up or down, and a combination of these. The balancing condyle makes a circular motion in the medial direction, while on the working side it simply rotates. This transverse rotational movement of the mandible can occur in two phases: immediate lateral translation of the mandible (LT) and its progressive lateral translation (LT).
Despite the contradictory considerations, the condyle on the working side cannot move (translate) laterally unless an LT condyle occurs on the balancing side. The corpus translation of the mandible is called Bennett's motion, and the angle of such is formed as the condyle on the balancing side advances during the motion, continuing the circular moment to the medial wall of the articular tubercle.
The arc of a circle becomes sharper when the radius of the circle decreases - this is logical. The intercondylar state is fixed and cannot be changed by unifying the movements of the condyles on the working and balancing sides. However, lateral displacement of the mandible essentially shifts the center of rotation, which is located in the projection of the condyle on the working side, and thus changes the positional relationship of the condyle on the balancing side. All this leads to a change, namely to a decrease in the intercondylar distance relative to the original center of rotation. In fact, the Gothic arch trace, represented graphically, becomes more lateral with less intercondylar distance. This effect is observed when simulating movements in the Hanau H2 articulator in order to simulate the rotational trajectories of the lower jaw. The condylar ball on the working side remains in the condylar fissure, while the intercondylar pin slides transversely through the ball.
Discussion
Occlusal balance can be described by the ratios of the parameters of the so-called Hanau five. The articular guide is fixed and patient-specific, while the incisal guide is determined by the physician to suit the patient's profile and needs. The main problem is that the clinician can correctly determine the location and inclination of the teeth located between the distal determinant of CH and the anterior determinant of RN. The Swanson formula presented above was proposed to numerically determine the inclination of the distal teeth in order to achieve occlusal balance during protrusion. In this formula, the NB is the sum of the angulation of the orientation of the occlusal plane, the compensation curve and, in fact, the NB. For example, a 30-degree NB can be reproduced by combining teeth with a 10-degree cuspal inclination with a 10-degree OP orientation and a 10-degree compensation curve. The BN level for all distal teeth is the same only when the PH is equal to the SN. However, this slope will change significantly along the OP, when the pH value exceeds or, on the contrary, falls below CH. The more anteriorly the tooth is located, the more pronounced the effect of RN becomes. Thus, premolars may exhibit higher rates of inclination compared to molars when the PH is significantly more acute than the SN (in degrees of angle). The d indicator in the Svenson formula is not constant, and, in fact, represents the weak point of this formula. It denotes the relative position of the tooth from the RN as the reference position to the two final-determining landmarks. Taking into account the individual variability in the sizes of the anatomical components of the dentofacial apparatus, the value of d remains unknown until the distance from the RN is determined. According to Christensen, the average value of d can be approximated as follows: 0.5 for the third molar, 0.4 for the second molar, 0.3 for the first molar, and 0.2 for the premolars. Swenson's formula is quite effective for determining occlusal balance in a protrusive state.
Excessive inclination of the pelvis can compromise the distribution of masticatory loads and, as a result, cause the development of a number of biomechanical problems regarding function and esthetics. In fact, OOP is largely determined by the anatomical features of the structure and functional relationships of the dentofacial apparatus. A prosthetic curve with an appropriate level of inclination can be included in the OOP design. This approach is based on the geometric concept of a sphere passing through the axis of the condyle and the point of the incisal edge. In essence, this method is anthropomorphometric, and may well be suitable for modeling OOP in order to achieve occlusal balance. At the same time, however, one should not forget about the optimal value of the compensation curve, which plays no less a role in the state of balanced occlusion. The morphological profile of the cusps can rise above the level of the OOP to fill the interocclusal space created by the effect of disocclusion of the distal teeth.
According to Christensen, the cusp height indicator can also be used to compensate for insufficient OP inclination. But in fact, the state of balance depends more on the inclination of the tubercle than on its height. NB, in fact, refers specifically to the angulation of the distal teeth, while the height of the cusp determines the range of occlusal contact during excursive movements of the jaw. The NB begins from occlusal contact in a state of central occlusion and serves as a kind of guideline for sliding the cusp of the antagonist tooth without disturbing the occlusal balance. The greater the height of the tubercle, the greater the range of balance. However, it should be remembered that the functional range of motion of the lower jaw very rarely reaches its marginal boundary values. Maintaining lateral balance is important due to the significant frequency of lateral movements of the mandible. The teeth are usually positioned to form a curve in the mediolateral direction. This mediolateral compensation curve usually involves a more apical position of the lingual cusps compared to the buccal cusps in the mandible. If the relationship between the positions of these tubercles is reversed, a reverse compensation curve is formed. Essentially, the compensation curve is designed to increase the balancing slope and decrease the operating slope. In this case, the decrease in the working inclination is a derivative of the function of increasing the balancing inclination (photo 7). This approach allows the conventional sphere of the dentofacial apparatus to cross the OOP in the lateral direction, since this is determined by the inclination of the cusps of the distal teeth.
Photo 7. Inclination of the cusps of the lower molars: balancing inclination - red line, working inclination - blue line.
Semi-adjustable articulators are characterized by a number of limitations in relation to the reproduction of the articular guide. The widely used articulator Hanau H2 is not able to take into account the so-called Fischer angle, which is defined as the difference between the horizontal and vertical components of the CH. The horizontal component determines the descending element of the condyle trajectory during protrusive movement, and the vertical component determines the descending element of the condyle trajectory on the balancing side during lateral movement. On the other hand, the occlusal error that arises as a result of not taking into account the Fisher angle may be clinically insignificant.
Certain articulators are unable to reproduce either a record of occlusal movements or provide a record of lateral interocclusal relationships. Such articulators are simply not designed to adapt the parameters of the intercondylar distance and individual movements of the condyle on the working side.
According to Weinberg, the significance of occlusal error increases with the cumulative influence of a number of factors that were incorrectly determined at the stages of planning and manufacturing the prosthesis. Occlusal errors during rehabilitation with complete removable dentures can be minimized if the differences between the values of NT relative to the actual ones are less than 0.2 mm, PT - less than 5 degrees, intercondylar distance - less than 5 mm, articular guide - less than 5 degrees. Positive occlusal errors can be corrected directly in the mouth. The maxillary model should be positioned with respect to the face bow, although the reference transverse horizontal axis may not be within a 5 mm zone of the true transverse horizontal axis. The facebow transfer procedure must also include adequate positioning of the anterior reference point. The intercondylar distance can be measured using a facebow. When this distance is greater than 110 mm, the correction level for lateral movement of the condyle is set at about 0 degrees to achieve lateral occlusion balance.
You should also take into account the parameters of motion and Bennett angle, which are important components of LT and PT. The influence of these factors limits the possibilities for using the Swenson formula to determine working and balancing slopes. Centric relation remains a key success factor in complete denture rehabilitation. This position is the starting position for balanced occlusion. The morphology of the cusps of artificial teeth should not limit the stages of the chewing cycle during movements of the lower jaw. Adjustments to occlusal relationships should be made until a state of complete freedom in the centric relation position is achieved, maintaining occlusal height and balance during functional movements of the mandible. When there is interference in the occlusion state, the maxillary palatal cusps are used as centric stops to recreate the concept of lingual contact occlusion. Dynamic stability of complete removable dentures simply cannot be achieved without the formation of a pattern of balanced occlusion through the relationships of the Hanau five components.
Photo 8. Balanced articulation during lateral excursions of the mandible: right working side.
Photo 9. Balanced articulation during lateral excursions of the mandible: left balancing side.
Photo 10. Balanced articulation during lateral excursions of the mandible: right balancing side.
Photo 11. Balanced articulation during lateral excursions of the mandible: left working side.
conclusions
The state of balanced occlusion, obtained through the functional relationship of the constituent parameters of the Hanau quintuple, can be represented using the Swenson mathematical formula. This formula allows you to approximate the protrusive inclination when the distance to a specific tooth is determined relative to the reference parameters RN and SN. However, to achieve proper working and balancing inclination, the individual characteristics of the trajectories of movement of the articular head, as well as the practical capabilities of the articulators, must be taken into account during the manufacture of complete removable dentures. The process of modeling the design of complete removable dentures is not ideal, therefore, during the fitting of the design in the oral cavity, various occlusal interferences can be recorded, which can be leveled directly clinically. The centric relation is the critical and starting position of the balanced occlusion pattern. Occlusal adjustments must take into account the basic principles of complete denture design, including the need to ensure freedom of movement of the mandible from the centric relation state, as well as proper vertical bite parameters.
Authors: Won-suk Oh, DDS, MS Berna Saglik, DDS, MS Sun-yung Bak, DDS
Functional significance of the tubercles
The buccal cusps of the upper and lower molars, as well as the lingual cusp of the lower molar, perform a protective function. The palatal cusp of the upper molar is the supporting one.
In the process of closing the teeth in the central position, contact occurs between the palatal tubercles of the upper teeth and the central fossae or marginal projections of the molars and premolars of the lower jaw. There is also contact between the buccal tubercles of the lower teeth and the central fossae and marginal projections of the molars and premolars located above.
Note! The buccal tubercles of the teeth of the lower jaw and the palatine tubercles of the upper are supporting and holding ones. The lingual cusps of the lower teeth and the buccal cusps of the upper teeth are guides and protective (prevent biting the cheek and tongue).
When performing chewing movements, the lower jaw should slide over the surface of the upper jaw teeth without obstacles. The tubercles slide smoothly along the antagonist slopes without disrupting occlusal relationships.
At the same time, they must maintain tight contact. Sagittal and lateral movements are reflected on the surface of the first molars of the mandible by the arrangement of transverse and longitudinal fissures, this is called the “occlusal compass”.
Important! This landmark is necessary in the process of modeling the occlusal surface of the teeth.
During the movement of the lower jaw forward, the guide tubercles of the chewing teeth of the upper localization slide along the central fissure of the teeth located below. During lateral movements, gliding occurs along the fissure that separates the median buccal and posterobuccal cusps of the lower molar.
In the process of combined movement, gliding occurs along the diagonal fissure that divides the median buccal tubercle. The “occlusal compass” is characteristic of all teeth of the lateral group.
“Occlusal compass” - A and C - sagittal movements, B and E - transversal, D - combined.
Another important factor in the biomechanics of the lower jaw is the height of the cusps of the chewing teeth. This parameter determines the amount of initial joint displacement.
This is due to the fact that during the lateral movements of the lower jaw, the head on the working side moves outward before the rotational movements begin, while the head on the balancing side moves inward. This type of movement occurs within 0-2 mm.
The greater the flatness of the slopes of the tubercles, the greater will be the magnitude of the initial articular shift. This is how the free mobility of the dentition relative to each other within the boundaries of central occlusion is determined.
Note! In the process of modeling artificial teeth, it is very important to take into account the characteristics of the tubercles, as well as the inclinations of the slopes of the chewing teeth. Otherwise, disturbances in the interaction of the elements of the TMJ are possible, that is, the progression of joint dysfunction.