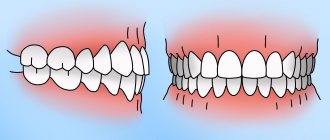
Mesial occlusion or occlusion is one of the types of defects in which the closure of the anterior dentition is disrupted. Outwardly, this manifests itself in the dominance of the lower jaw over the upper. With such a violation, not only an aesthetic defect is observed. This leads to abrasion of tooth enamel and changes in facial expression. Typically, malocclusion develops due to genetic predisposition or exposure to causative factors during a certain period of development.
Mesial occlusion can be corrected professionally. A competent approach, modern equipment and doctors will be able to restore the aesthetic appearance of the face. Dental clinic PROPRIKUS provides treatment of mesial occlusion without the use of surgical intervention. To correct malocclusion, we use aligners, including Invisalign. They are considered the most effective and help correct even complex cases of pathological occlusion.
Symptoms and causes of mesial occlusion
Patients with this pathology have a concave profile: the lower part of the face is increased in size due to a sharply protruding chin. The lower lip appears thicker than the upper lip, and the jaws are not closed properly. The lower row of teeth is pushed forward. In addition to external manifestations, deformation affects functionality:
- speech is disrupted;
- difficulty biting and chewing food;
- sometimes an open or crossbite develops.
Due to uneven load on the incisors of the jaws, early tooth loss is possible. In 50% of cases, the cause of the anomaly was disturbances in fetal development in the prenatal period. Among the main factors influencing the formation of malocclusion are: birth injuries, viral infections during pregnancy, rickets, osteomyelitis, incomplete development of the dentition. Today, the PROPRICUS clinic successfully corrects mesial occlusion in both adults and children of all ages.
Need some advice?
Enter your phone number and we will give you a free consultation
I want a consultation
*By making an appointment you consent to the processing of your data
Diagnostics
To confirm and clarify the diagnosis for the correct treatment of prognathia, the following methods are used.
- functional Eschler-Bittner test (after moving the lower jaw forward, the doctor assesses whether the profile has improved or worsened: in the first case, the cause of prognathia is the underdevelopment of the lower jaw, and in the second, the size of the upper jaw is too large);
- radiography;
- photographing the face from the front and profile;
- taking dental impressions [1, 2].
Methods for correcting mesial occlusion in adults
Mesial occlusion, which is detected before the age of 12 years, is more treatable. Unfortunately, this does not always happen and often adult patients seek help in correcting their bite. Conservative orthopedic methods for correcting occlusion are sometimes ineffective. Often teenagers and adults complain of pain and discomfort when installing a corrective structure. But at the PROPRICUS clinic they use the most effective methods. Serious defects can be corrected with veneers, aligners, and mouth guards. We treat mesial occlusion in adults even in the most difficult situations, when it seems that it is impossible to return the teeth to their normal appearance.
Classification
By severity:
- Gnathic form. Develops due to improper development of the cranial bones.
- Dentoalveolar. It is formed when the tooth roots are incorrect or when there are significant differences in the sizes of the lower and upper jaws.
The pathology may have a mixed form.
By localization:
- General. The defects extend to both the front and side elements.
- Partial. The anomaly concerns the front teeth.
By etiology:
- True progeny. The anterior and posterior teeth have an irregular position, with space present between the anterior units. Pathology reduces the functional abilities of the dentofacial apparatus, and protrusion of the movable jaw brings psychological discomfort.
- False. Affects only a few frontal units. The anomaly is more common in elderly patients and may also be a consequence of improper surgical treatment.
Types of mesial occlusion
Pathology is classified depending on the cause of origin and form.
There are the following types of occlusion in form:
- Dentoalveolar - accompanied by incorrect position of the teeth, corrected with the help of orthodontic structures;
- skeletal form - refers to more complex forms; malocclusion is formed due to pathology in the development of the jaws.
By nature of occurrence:
- micrognathia of the jaws - characterized by their increase or decrease in size;
- prognathia of the lower jaw - normal closure of the jaws is impossible due to individual teeth;
- retrognathia - characterized by a normal jaw size, but its incorrect position;
- macrodentia and microdentia.
If parents are diagnosed with this disorder, then it is necessary to carefully monitor the condition of the child’s teeth. Genetic predisposition and exposure to adverse factors increase the risk. It is important to take your child to see a dentist every six months. Early loss of primary incisors due to trauma or caries is dangerous for the development of mesial occlusion in the future, even with correct occlusion. The pathology can be noticed at an early age - by an enlarged lower jaw and lower incisors overlapping the upper ones.
What exactly should you do if the baby has prognathia : the chin is absolutely not “strong-willed”, the lower jaw “crawled” back, and the upper teeth, like those of a rabbit, protrude forward? Exercises for the lips and lower jaw - myogymnastics, are carried out in parallel with breathing exercises and wearing a vestibular plate (with the visor pointing down). Naturally, during myogymnastics the plate should not be in the baby’s mouth. The exercises are done 2-3 times a day, first for 5 minutes, then for 10-15 minutes, sitting in front of a mirror. Do not take the whole complex at once to work with your child. Start with one or two exercises. When you get good at them, master the next ones, but don’t forget to repeat the previous ones. And it would be a good idea to visit a speech therapist before starting self-study at home.
1. Exercise “Smile”. The lips smile naturally, the teeth are clenched in a “fence”, i.e. The upper teeth “stand” above the corresponding lower ones. The front teeth are clearly visible. Maintain this position for at least 10 seconds (the time lengthens from activity to activity).
2. Exercise “Tube”. The teeth are tightly clenched. Pull your lips forward with a tube and hold in this position for at least 10 seconds (the duration gradually increases).
3. Alternate exercises “Smile” - “Pipe” at the count of “one-two” at least 10-15 times. Teeth are clenched all the time! Take your time! Fix one or the other position of the lips.
4. Exercise “Fish” . The teeth are clenched tightly, the lips are extended forward (see exercise “Tube”). The lips open and close (as a fish does with its mouth in an aquarium).
5. Exercise “Funnel ”. Move the lower jaw forward, open the mouth slightly, and open the teeth. On the count of “one”, pull your lips forward with a “horn”; on the count of “two”, pull your lips inside your mouth, tucking them behind your teeth (the lower jaw is still pushed forward!). Do at least 10 repetitions.
6. Exercise “Annoyance”. Bite your upper lip with your lower front teeth at least 10-15 times. Hold this position for 5-10 seconds. The lower jaw is pushed forward as much as possible.
7. Exercise “Timpani”. The lips are slightly curled behind the teeth inside the mouth. Slap them one against the other, making a characteristic patting sound. The lower jaw is pushed forward as much as possible. Do this at least 10 times.
8. Exercise “Snorting horse ”. Relax your lips and snort, like a horse does. Move the lower jaw forward as much as possible. Do this at least 10 times.
9. Exercise “Deadbolt”. Move the lower jaw forward as much as possible. Move it from side to side at least 10-15 times with maximum amplitude.
10. Exercise “Hide and Seek”. a) “Hide” the upper lip by biting it with the lower front teeth. Only the lower lip is visible, it stretches up towards the nose. Hold in this position for at least 5 seconds (the time to complete the exercise increases from session to session);
b) “Hide” the upper and lower lips, drawing them into the mouth and slightly squeezing them with the front teeth. The lower jaw is pushed forward as much as possible. Hold in this position for at least 5 seconds (the time to complete the exercise increases from session to session).
11. Exercise “Plane” . “Cross” the lower central incisors along the upper lip at least 10-15 times. The lower jaw moves forward and “works” energetically.
How to eliminate progeny?
Correcting progeny (the lower jaw protrudes unnaturally) can be difficult. But regularly wearing a vestibular plate (with the visor pointing upward) and performing articulation exercises (myogymnastics) help cope with this malocclusion.
The child needs to imagine that his teeth and lips are “stubborn doors” that always strive to “skew.”
1. Articulation exercise “Aligning the doors” : a) open your mouth slightly, then, slowly moving the lower jaw back, place the edges of the lower central teeth on the edges of the upper ones, hold this position for 5-10 seconds;
b) open your mouth, then, moving the lower jaw back, compress your lips tightly, slightly biting them with your teeth, hold for 5-10 seconds.
What should you do if one door leaf prevents the other from closing? That's right, take a plane and remove all the “unnecessary”!
2. Exercise “Plane” : “Cross” the upper central teeth along the lower lip at least 10-15 times. The lower jaw moves back and actively “helps” in this work.
3. Exercise “Rabbit”: a) bite the lower lip with your upper front teeth at least 10-15 times. Then grab your lower lip with your upper teeth and hold this position for 5-10 seconds. The upper front teeth are clearly visible during this exercise.
b) try to reach the upper part of the chin with your upper incisors and also lightly bite it. Fix this low position of the upper jaw on the chin and hold it for 5-10 seconds. The upper front teeth are clearly visible.
And now he will play hide and seek with his lips and teeth.
4. Exercise “ Hide and Seek ”: “hide” the lower lip behind the upper front teeth and the upper lip, biting it. In this case, only the upper lip is visible, it seems to hang over the chin, but the upper teeth are not visible. Hold in this position for at least 5 seconds (the time increases from session to session.
With the help of articulation exercises and plates, the child acquires useful skills that help him cope with the pronunciation of difficult sounds, and he develops a correct bite. But you have to be prepared for the fact that wearing the plates and producing sounds will last for several years. This will require enormous patience from parents and children.
Causes of mesial bite
In the early stages of development:
- genetic predisposition - congenital anomalies in the structure of the skull and facial bones occur;
- illnesses suffered during pregnancy, deficiency of vitamins and nutrients, living in unfavorable conditions;
- increased size of the child's tongue;
- pathologies of the thyroid gland, rickets;
- short frenulum, improper breastfeeding.
During the period of milk and permanent teeth:
- insufficient wear of primary teeth in children 3-6 years old;
- premature loss of teeth in the upper jaw due to caries or impact;
- late appearance of teeth on the upper jaw;
- bad habits - resting your chin on your hand, sleeping in a position with your head bowed to your chest.
Most often, abrasion is disrupted on temporary canines due to the late period of physiological change. This prevents the closure of the dentition, and therefore mesial occlusion is formed. The correction scheme depends on the severity of the deformity. Therefore, PROPRICUS dentistry uses several treatment methods. The patient undergoes a detailed diagnosis by several specialists to understand how to correct the mesial bite.
Consequences of distal occlusion
If left untreated, distal occlusion leads to a variety of problems and significantly impairs quality of life. In particular, with a deep distal bite, the following disorders are typical.
- Due to improper distribution of chewing load, bone structures are deformed.
- Chewing and swallowing are impaired, since the dentofacial apparatus works ineffectively, with a predominance of grinding and crushing movements.
- The cutting edges of the teeth come into contact with the mucous membranes of the gums and palate, causing the soft tissues to become damaged and inflamed. As a result, stomatitis, gingivitis or even oncology may develop.
- The back teeth are overloaded and quickly destroyed. Chips and cracks appear on their protective shell, which develop into caries.
- Oral hygiene deteriorates. More hard-to-reach places appear where dental plaque accumulates.
- Improper functioning of the temporomandibular joint leads to discomfort when speaking and eating.
- The proportions of the face are distorted, its harmony is disrupted.
- Speech becomes slurred.
- Prosthetics are becoming more complicated [2].
Methods for treating mesial occlusion
Aligners are one of the most practical, convenient, safe and effective correction methods. They are made from polymer materials according to the patient’s individual impression. Therefore, the risk of the structure shifting is completely eliminated. Aligners follow the anatomical shape of the teeth and jaw. They cannot be seen on the teeth due to the complete transparency of the trays. Patients observe minor defects within 2-3 days after installation. They do not interfere with chewing, drinking, or brushing your teeth. You should remove your aligners before performing oral hygiene and eating.
Sign up for free 3D modeling of your future smile!
Make an appointment
*By making an appointment you consent to the processing of your data
Advantages of aligners:
- do not stain;
- not visible to others;
- soft and elastic;
- safe for health;
One of the most advanced foreign bite alignment systems is Invisalign. This is an innovative product from an American company that is used in our clinic. Therapeutic mouth guards create pressure on the teeth, causing them to return to their normal position. We use only original products and are completely confident in the effectiveness of orthodontic treatment with aligners.
During the initial examination, the doctor assesses the condition of the patient’s oral cavity, diagnoses the condition of the jaw system, draws up a treatment plan and names its cost. Before the treatment plan is approved, the patient is shown what the oral cavity will look like after treatment. After agreeing on the details and signing the contract, the doctor performs sanitation of the oral cavity, if there is an indication for this. Therapeutic mouth guards take 2 weeks to make. The elements will have to be changed and will have to be changed every 2-3 weeks. The average duration of treatment with aligners is 6 months to 1.5 years.
Why is progeny dangerous?
With progenia, the process of chewing, digesting and assimilation of food is disrupted. A person with a severe pathology experiences difficulty while eating, sometimes even cannot take a full bite, which leads to increased stress on the gastrointestinal tract.
There is a redistribution of the load on the teeth, as a result of which some of them wear out faster and require frequent treatment. In addition, the proportions are disrupted and the appearance of the face changes. Such an aesthetic defect in childhood can cause complexes and isolation in a child.
Impairments in oral breathing also appear. The consequence of this is an increased incidence of colds, periodic chapping of the lips and dryness of the oral mucosa.
Correction of bite during progenia
The choice of correction methods depends on the type of pathology and the causes of its occurrence. The orthodontic appliances used stimulate the development of the upper jaw and correct the position of the teeth. DaVinci studio dentists use:
- mouthguards;
- trainers;
- plates.
These are less painful and long-lasting methods of correction. When starting treatment in adulthood, the braces system will help you achieve the desired result. Children wear them from one to one and a half years, while adults wear them for about four years.
Serious dental deformities in the absence of a desire to use braces are treated with surgical intervention in adulthood. Surgery is a financially expensive method associated with the risk of complications. Therefore, if a dentist recommends wearing orthodontic appliances, it is better to listen to the advice.