Salivation is a natural physiological process that occurs throughout a person’s life. Special glands located in the oral cavity are responsible for it.
They are capable of producing about 2 liters of saliva per day. Sometimes the amount of saliva produced increases sharply, which significantly affects the quality of life. This is especially common in childhood.
Increased salivation in a child can be caused by various reasons, both natural and pathological. To understand this issue, it is necessary to consider what role saliva plays in the life of a child’s body.
Functions of saliva
Firstly, it is involved in the digestion of food, making it softer and helping it move through the esophagus. The enzymes contained in saliva are capable of breaking down starch and fats. Thus, food enters the stomach already partially digested.
Secondly, saliva plays a protective role, preventing the mouth from drying out and having a bactericidal effect. It helps to wash away food debris, and with it bacteria. Saliva neutralizes many acids and alkalis, protecting tooth enamel from their aggressive effects. It is also able to strengthen the enamel, nourishing it with important microelements (fluorine, phosphorus, calcium).
Thirdly, it helps make teething less painful by reducing inflammation in the gums. And finally, in the first months of a baby’s life, saliva has a special viscosity, which makes breastfeeding easier during natural feeding.
Causes of increased salivation in children
Excessive drooling is scientifically called hypersalivation. In children, there are clearly visible age periods when it can occur most intensely.
Important! There is a distinction between true and false hypersalivation.
True hypersalivation is caused by malfunctions of the salivary glands, and false hypersalivation (also called reflex) in childhood is associated with more serious disorders in which swallowing saliva becomes less frequent.
For example, if the sensorimotor arc malfunctions, the interaction between the brain and the oral cavity is difficult. The child's number of spontaneous swallows is reduced, which creates the appearance of profuse drooling. Depending on the age, the causes of increased salivation in children may be different.
Causes of drooling can be physiological and pathological
Beginning ARVI
Sometimes excessive salivation, accompanied by regular attempts by the baby to put his fingers and fists in his mouth, indicates the onset of an infectious disease such as ARVI, flu, sore throat, etc. In this case, the child has a fever, nasal congestion or mucus discharge from the sinuses. Many babies begin to sneeze and cough.
The main function of saliva is protection against pathogenic microbes and bacteria. This is what causes the increased activity of the salivary glands in babies 2-4 months of age against the background of the onset of ARVI and other inflammatory processes localized in the oral cavity.
In this case, the main help lies in the fight against the causative agent of the disease. The cleanliness of the baby’s hands, pacifiers and toys should be taken with special care during this period, as there is a high risk of harmful microorganisms being introduced into the baby’s body.
Newborn period
In newborn babies, salivation is normally absent due to the underdevelopment of the salivary gland apparatus. However, often a mother may notice how, in the first hours of a child’s life, a colorless liquid, very similar to saliva, is actively secreted from his mouth.
Most often, this is how amniotic fluid comes out, which the baby managed to swallow while passing through the birth canal. Normally, this phenomenon should stop a few hours after birth. If drooling continues longer, it is better to inform your pediatrician (neonatologist) about this in order to exclude serious health problems.
Pediatrician appointment prices:
| TYPES OF MEDICAL SERVICES | Cost, rub. |
| Examination of a child by a pediatrician to obtain a certificate + certificate | 1950 |
| Visit of a pediatrician, consultation at home (Moscow) | 5400 |
| Consultation with a pediatrician at home for the second child | 1950 |
| Patronage for a newborn / gymnastics and swimming at home (1 session, pediatrician Kapina A.V.) | 6300 |
Drooling at 2–3 months
At the age of about 2 months, a baby may experience profuse salivation, caused by the fact that the salivary glands finally begin to work at full capacity. It is at this age that a child may need his first bib to protect his clothes from getting wet.
The mother also needs to very carefully monitor the condition of the child’s skin, especially the area around the lips and chin. Excessive saliva can irritate baby's delicate skin. To prevent this from happening, it is recommended to lubricate the area around the mouth with baby cream or Vaseline.
Inflammation of the submandibular salivary gland
Closer to 3 months, children become active explorers of the world around them and taste everything. They put fingers, toys and any other objects at hand into their mouths.
The baby's body becomes acquainted with new microflora, which leads to increased secretion of saliva, which performs a protective function. At this age, increased saliva production can also occur against the background of an acute respiratory disease.
Breathing through the nose becomes difficult, and the child has to breathe through the mouth. This causes the nasopharynx to dry out and reflexively release a larger amount of saliva than usual, which moisturizes the air and disinfects it.
The child is drooling: what to do?
An average person produces between 500 ml and 2,000 ml of saliva per day. It plays an important role in our body: moistens food, promotes chewing and swallowing, moisturizes the tongue and lips during conversation, promotes normal speech, cleans teeth and gums and maintains normal oral hygiene. Saliva regulates acidity in the esophagus (saliva has an alkaline pH), destroys microorganisms and cleanses toxic substances, enhances the perception of taste, and begins the digestion of carbohydrates (contains enzymes for this). However, with some diseases, the amount of saliva increases and it flows out of the mouth, which, in turn, causes discomfort.
Why this happens and what to do about it, we figure it out with Natalya Savva, Candidate of Medical Sciences, Associate Professor, Director of the Children's Palliative Charitable Foundation for scientific and methodological work.
What is drooling?
Saliva leaking from the mouth can occur when:
- Increased production of saliva (hypersalivation).
- Impaired swallowing of saliva and sputum (impaired lip closure and impaired swallowing - dysphagia).
Each child has its own reason or combination of these factors. Therefore, to select the correct treatment, you need to find out what underlies drooling in each child individually.
Do healthy children drool?
Typically, drooling occurs in children under one year of age (the peak occurs at 5-6 months). This age-related feature completely disappears by the age of two - by this time the child’s oral cavity has functionally matured.
In addition, increased salivation in children occurs when their teeth grow, they are in psycho-emotional agitation, if they feel sick and vomit.
Drooling can occur due to the taste or smell of food, spices, acid, pleasant or unpleasant physical and emotional stimuli, as well as in anticipation of food or fear of pain.
What can cause or worsen drooling?
Diagnosis of swallowing dysfunctions What are the main signs of dysphagia, when is it necessary to test using the three-swallow test method Kristina OsotovaCaring Workshop
Nursing
Causes of drooling or its intensification can be:
- Loss of drool control.
- Inadequate lip closure and open mouth.
- Impaired or lack of sensitivity in the oropharynx.
- Impaired tongue movement.
- Impaired tone of the tongue and lips.
- Dysphagia (impaired frequency of swallowing and difficulty swallowing).
These conditions may cause or worsen positional problems (poor head and neck control), problems with teeth and dental structures, and the use of medications (eg, for the treatment of epilepsy).
What diseases cause increased salivation?
There are diseases in which drooling increases: temporarily or chronically, depending on whether the cause of drooling can be treated.
Increased saliva production and/or impaired saliva retention in the mouth occurs when:
- Organic lesions of the central system (cerebral palsy (CP), trigeminal facial palsy, neurodegenerative diseases of the central nervous system). Most children with cerebral palsy have impaired swallowing and control of saliva flow; they cannot close their lips while swallowing. Impaired swallowing of saliva is affected by spasticity and muscle dystonia: this causes problems with tongue control, high tone of the tongue and muscles of the oropharynx, spastic contraction of the upper esophageal sphincter, and poor coordination between the pharynx and this sphincter. In addition, the loss of control over holding the head and neck affects swallowing disorders.
- Neuromuscular diseases (spinal muscular atrophy, Duchenne muscular dystrophy, myopathies, myasthenia gravis, myositis). In neuromuscular diseases of muscle tone (for example, SMA, Duchenne muscular dystrophy), salivation occurs due to increasing atony of the muscles of the lips, oropharynx, esophagus, stomach, intestines, the addition of gastrostasis (delayed gastric emptying) and gastroesophageal reflux.
- Cognitive and mental disorders. Drooling can develop due to delayed psychomotor development (impaired formation and development of swallowing movements, ineffective and infrequent swallowing, incomplete closure of the lips during swallowing).
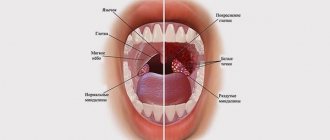
- Diseases of the ear, nose and throat. Acute infectious processes of the oral cavity and pharynx (gingivitis, stomatitis caused by viruses, bacteria, fungi) cause damage to the mucous membrane, as well as pain and problems with swallowing. This causes drooling, for example, with tonsillitis, peritonsillar or retropharyngeal abscess, epiglottitis.
- Diseases of the gastrointestinal tract, esophagus (gastro-esophageal reflux, gastroparesis, gastrostasis, pancreatitis).
- Familial autonomic dysfunction (Riley-Day syndrome), Wilson's disease, Rett syndrome.
- Vitamin B3 deficiency.
- When taking medications. Hypersalivation is caused by various drugs: antiepileptics (clonazepam), painkillers (morphine), pilocarpine, haloperidol; benzodiazepines.
How is drooling treated?
- Conservative non-pharmacological therapy
How to properly treat the oral cavity of a seriously ill patient We show exactly how and in what positions you can brush your teeth Kristina OsotovaCaring Workshop
Care
It is important to promptly identify and begin treatment for the cause of drooling, monitor oral hygiene, regularly brush your teeth, and remove plaque. It is advisable to replace medications that cause or increase salivation (only after consulting a doctor). Take your child to the dentist more often - every 4-6 months.
Physiotherapy will improve jaw closure and tongue function, develop tongue mobility, strength and placement in the oral cavity, and improve lip closure, especially during swallowing. Positioning and swallowing development (speech therapy massage) are also helpful.
If a child has moderate drooling, normal or nearly normal intelligence, and is highly motivated to stop drooling, behavioral or biofeedback therapy may help. The correctness of swallowing is monitored by parents or using special computer programs.
To prevent saliva from irritating the skin or if maceration occurs (swelling and wrinkling of the skin from prolonged contact with water), use a barrier cream or ointment.
- Pharmacotherapy
Important: Drugs are started with minimal doses and increased to maximum doses carefully depending on the clinical effect.
- Anticholinergic drugs - atropine, benzatropine mesylate, scopolamine, hyoscine - reduce the volume of saliva. But they may have side effects: blurred vision, dry mouth, constipation, urinary retention.
- Scopolamine or hyoscine patch (in the photo - behind the child’s ear). They last 48 or 72 hours and are glued to the skin behind the ear.
- Glycopyrrolate is a long-acting medicine (8-12 hours) with minimal side effects. The drug is 5-6 times more effective than atropine, effective in 90% of patients with hypersalivation.
Photo by Alexandra Glagoleva
- Botulinum therapy
Botulinum therapy is used to treat muscle spasticity, for example, with cerebral palsy. The medicine blocks nerve impulses in the muscles, sweat and salivary glands. In case of drooling, the medicine is injected directly into the salivary gland under ultrasound control and local anesthesia in a day hospital (24-hour observation is not required).
The therapy consists of four injections, which are placed in the submandibular and parotid glands. On average, salivation decreases for 6 months. Side effects are minimal and usually occur at the injection site. Speech and swallowing may be slightly impaired.
- Surgery
Surgical treatment is prescribed for children over 6 years of age with profuse uncontrolled drooling (if conservative therapy has no effect within 6 months).
There are different types of surgical procedures to treat drooling (eg, deinnervation of the salivary gland, excision of the salivary gland (eg, submandibular), ligation of the salivary gland duct, etc.). The operation lasts 60-90 minutes, requires general anesthesia and a 24-hour hospital stay for several days.
When excision of the salivary glands there is a high risk of damage to nearby nerves and paralysis of the muscles that this nerve innervates. Side effects early after surgery may include bleeding, swelling, infection, and difficulty swallowing.
Complications of drooling
Drooling is a cosmetic defect. It can lead to social isolation and have very severe psychological consequences for the child and the entire family. Drooling can cause emotional and physical discomfort in a child. Children with drooling can soak not only their own toys and books, but also the things of those around them, which is especially negatively perceived in public places and organized children's groups. Severe drooling increases the burden on parents: they need to constantly change things and blot the saliva.
Drooling contributes to the spread of infection, loss of fluid and electrolytes, and in severe cases can cause dehydration (dehydration), deterioration of articulation and speech.
How to dress a child with severe drooling?
Adaptive clothing for children What clothes can be chosen for children with contractures and prostheses, and why teenagers with disabilities want to look like ordinary kids Katerina Pechurichko
Palliative care for children
Bibs and scarves
If drooling is severe, use waterproof bibs (for example, silicone ones with a pocket for collecting saliva or double ones with a waterproof bottom layer). An older child can wear a beautiful saliva-absorbing colored scarf with a pattern over the bib (so getting wet is less noticeable). Stock up on several scarves of the same color: this way you won’t notice their replacement (you need to change scarves often so that bacteria don’t multiply and things don’t smell).
Vests
If your clothes get wet, it is often inconvenient to change them: wear vests over your clothes, which are easy to remove and change when they get wet. You can use windbreaker fabric to make the vest get wet more slowly.
Velcro
Collars and other parts of clothing may have Velcro, which can be quickly unfastened and allow you to quickly change clothes, even in public places.
Created using a grant from the Absolut-Help Charitable Foundation
Stock image used from Depositphotos.
Teething period
Teething usually begins around 6 months of age. The child becomes whiny and irritable. The process of tooth extraction is accompanied by pain and the formation of wounds on the gums. They can greatly disturb the baby, bringing him a lot of suffering.
Salivation helps make pain less intense: saliva has an anti-inflammatory and calming effect. Teething is greatly extended over time and sometimes lasts up to 2 (and even 3) years.
Important! Increased salivation up to 2 years of age is most often caused by natural causes and is physiological.
Increased salivation after 5 years
If a symptom bothers a child at an older age, after 5 years, then this may be a cause for concern on the part of the parents. There are a number of reasons why saliva is produced in large quantities:
- inflammation in the oral cavity (stomatitis, gingivitis, candidiasis);
- infections of the upper respiratory tract and nasopharynx (for example, with adenoids, copious amounts of saliva are produced at night and prevent the baby from sleeping);
- disturbances in the gastrointestinal tract (gastritis, duodenitis, pancreatitis);
- helminthic infestations;
- poisoning with drugs, as well as toxic substances and household chemicals (a life-threatening condition - requires immediate medical attention);
- diseases of the nervous system (especially with damage to the central nervous system, some forms of cerebral palsy, congenital malformations).
If there is increased drooling of any etiology, it is best to show the child to a doctor. Only he will be able to determine the true cause of the symptom and, if necessary, prescribe additional examinations.
How to help muscles?
Exercises for the speech apparatus are useless while the muscles are too relaxed or, conversely, tense. Therefore, before classes you should massage the facial, neck and shoulder muscles. First of all, these are light strokes; sudden movements cannot be made. Lay your baby down so that his head is on your lap, at right angles to your chest. Movements are made with both hands on both sides of the face simultaneously in the following directions:
- from the middle of the forehead to the temples;
- from eyebrows to hairline;
- from the middle of the forehead along the cheeks to the neck and shoulders;
- from the earlobes through the cheeks to the nasal wings;
- from the corners of the mouth, first to the middle of the upper lip, then to the middle of the lower lip, then to the wings of the nose.
If the muscles are very tense, then the movements should be very light all the time, but if they are relaxed, then vigorous kneading and gentle stroking should be alternated.
This is general advice for parents of children with dysarthria. Specific sets of games and exercises and medications, if necessary, are selected only by a speech therapist and a neurologist, based on the characteristics of the child’s condition.
Publication date: 10/03/2019. Last modified: 01/13/2020.