Cheek cancer is a malignant neoplasm of the oral cavity.
Examination of patients with symptoms of cheek cancer at the Yusupov Hospital is carried out using modern diagnostic equipment from leading companies in the USA and European countries. Oncologists provide comprehensive treatment for cancer of the buccal mucosa. The medical staff is attentive to all the wishes of the patient. Chefs provide special dietary meals. Professors and doctors of the highest category develop tactics for managing patients with cheek cancer at a meeting of the expert council. Early diagnosis of the disease and multidisciplinary therapy improve the prognosis and five-year survival of patients after treatment.
Causes of cheek cancer
Cancer of the buccal mucosa develops under the influence of the following provoking factors:
- Use of tobacco in any form (cigarettes, cigars, pipes, chewing tobacco);
- Alcohol abuse (the risk of developing cancer increases when the use of alcohol and tobacco is combined);
- Infection with carcinogenic forms of human papillomavirus.
One risk factor is exposure to sunlight. Both family history and genetic predisposition, as well as exposure to mutagenic environmental factors, play a role in the development of cheek cancer. The formation of a malignant tumor occurs in several stages. The most important is the disruption in the functioning of oncogenes and genes that inhibit tumor growth. The development of malignant neoplasms of the cheek is associated with inactivation of the p16 gene, mutations in the p53 gene, and the introduction of the human papillomavirus.
Features of the appearance of bumps on the gums
The formation of a lump on the gum occurs as a result of the development of a pathological process, the cause of which may be a non-infectious or infectious process. In most cases, the formation is a “bag” of pus, but compaction from periodontal tissue cannot be ruled out.
A lump on the gum can be caused by pathogenic bacteria (infectious origin) or tissue trauma (non-infectious). The pathological process is also distinguished by the nature of its course: chronic and acute.
Mostly, an acute form of pathology initially develops with the manifestation of pain and signs of inflammation. If left untreated, the formation can lead to complications or become chronic with periodic relapses. Treatment for a chronic gum lump may require surgery.
The mechanism of development of cheek cancer
Malignant tumors of the cheek occur against the background of precancerous changes in the epithelial and subepithelial layers (leukoplakia or erythroplakia). The risk of leukoplakia degenerating into invasive cheek cancer is about 4-6%, with erythroplakia it reaches 30%. Subsequently, dysplasia transforms into “cancer in situ”, which penetrates into surrounding tissues and metastasizes to local and regional lymph nodes.
In some patients, even those cells that do not initially raise suspicion of dysplasia upon initial microscopy may gradually become malignant. As the tumor process progresses, distant metastases occur in the bones, lungs, and liver. Buccal cancer can grow through the skin.
Adenoid cystic carcinoma of the buccal mucosa
Adenoid cystic carcinoma (AC) is a malignant neoplasm of the salivary glands. The pathology was first described as Billroth cylindroma in 1856. The term adenoid cystic carcinoma was established in 1928 and is still used today. Adenoid cystic carcinomas account for less than 1% of all malignant tumors of the head and neck, and 50% of AKs arise in the oral cavity, mainly on the hard palate. Other slightly less common sites include the lower lip, retromolar/tonsillar region, sublingual gland, buccal mucosa, and floor of the mouth. Adenoid cystic carcinoma is clinically characterized by small size and slow growth. However, AKs spread invasively into surrounding tissues and form distant metastases. Pain is an important symptom for determining perineural extension. Thus, AKs have a long clinical course and a questionable prognosis, and the prognosis is somewhat worse when the minor salivary glands are affected than the large ones. We provide a description of the features of adenoid cystic carcinoma of the buccal mucosa in parallel with a review of the available literature.
Clinical case
A 45-year-old woman came to the clinic with complaints of a painful swelling on the mucous membrane of the left cheek. The formation was first noticed 3 months ago, after which it gradually increased in size. The appearance of the pathology was accompanied by pain, unexpressed and prolonged. An intraoral examination revealed a swelling with unclear boundaries on the mucous membrane of the left cheek in the area of the molars (photo 1). Palpation revealed a soft, well-defined, mobile swelling measuring 1x1 cm. The mucous covering the formation was not changed.
Figure 1: Intraoral photograph showing swelling in the left posterior buccal mucosa (black stripe).
OPG did not reveal any violations of the bone structure of the upper and lower jaws (photo 2). Ultrasound showed a hypoechoic mass with a homogeneous internal structure and defined edges. No calcification zones were found, the formation is not fused with the surrounding structures (photo 3). These features indicated well-defined, benign tissue masses. The formation was surgically excised. Histopathological examination revealed a violation of cellular architecture and a lattice structure of tumor cells with many small cystic cavities. Perineural invasion was detected (Figure 4). Based on the above symptoms, a diagnosis of adenoid cystic carcinoma was made. Since the edges of the wound were not affected, it was decided not to use auxiliary therapy. The patient remained under observation for 3 years without signs of relapse.
Photo 2: OPG without bone tissue pathology
Figure 3: Ultrasound image showing a clearly visible hypoechoic mass with a homogeneous structure (lesion marked with x)
Photo 4: X10 micrograph showing the lattice structure of tumor cells
Discussion
Adenoid cystic carcinoma is a rare epithelial tumor that is characterized by painlessness and constant growth. WHO defines adenocarcinoma as a basaloid tumor containing epithelial and myoepithelial cells in various morphological configurations, including tubular, cribriform and solid structures. This disease has a more severe clinical course and is usually fatal.
AK usually occurs in the 4th-6th decade of life with a predominance of women in the ratio of 3:2. In our clinical case, a 45-year-old woman suffered from the disease. Among all salivary gland neoplasms, 9–23% arise intraorally, 50% of which are malignant.
Most articles in the literature describe cases of adenocarcinomas of both minor and major salivary glands. However, there is practically no mention of damage to the buccal mucosa alone. This article is the first in this aspect of all 41 published works. After the overall analysis, 2280 cases of adenoid cystic carcinoma were found in 41 articles. Of this number, 1382 describe intraoral localization and 178 involve the oral mucosa. Based on the data presented, we can conclude that among the minor salivary glands, the buccal mucosa is affected in 12.9%. The overall percentage of adenoid cystic carcinoma in the cheek area is 7.8%. According to a review of all articles, 60.6% of all adenocarcinomas occur in the oral cavity.
The clinical manifestation of the tumor is slow growth and the formation of a dense mass. Pain is a common and important symptom, sometimes appearing before clinical manifestation. The pain syndrome is usually dull and prolonged. The described case presents a slowly growing painful swelling. Local lymph nodes are rarely involved. Hematogenous spread occurs in late stages of the disease. Distant metastasis usually occurs to the lungs, bones and soft tissues.
Histologically, adenoid cystic carcinoma occurs in three types: cribriform, tubular and solid. The tubular form is the most favorable, and the solid form is the most malignant. AKs are divided according to their histological nature into levels: I, II, III. Level I: combination of cribriform and tubular, level II: combination of cribriform, tubular and solid and level III: solid type only. The reported clinical case was of the cribriform type and classified as level I. The tendency for perineural spread is quite typical for AK. Common pain syndrome may to some extent be associated with this factor. However, it cannot be considered pathognomic. Such distribution cannot be considered prognostically significant, while some authors indicate that this parameter may be a sign of distant metastasis.
Various treatment options for AK have been proposed, including surgery, radiotherapy, chemotherapy and combination therapy. Surgical wide excision is the treatment of choice. In this case, this particular method was used. The prognosis of the disease can be influenced by a variety of factors. Tumor stage, excision margin, location, perineural invasion, solid histologic type, and presence of cervical lymph node metastases are also taken into account. AK usually has a long clinical course with the formation of distant metastases in the later stages of the disease. According to one study, the average time between diagnosis of the primary lesion and detection of distant metastases is 60 months, ranging from 18 to 120 months. Unlike other malignant tumors, adenocarcinomas usually do not lead to death in the short term, but at the same time have low long-term survival.
Conclusion
Adenoid cystic carcinomas are seemingly harmless lesions that are characterized by very slow growth. However, due to the tendency for perineural spread and distant metastasis, this pathology requires careful and long-term observation.
Authors: Vidya Ajila , Department of Dentistry and Radiology, AB Shetty Memorial Institute of Dental Sciences, Nitte University, Deralakatte, Mangalore Shruthi Hegde , Department of Dentistry and Radiology, AB Shetty Memorial Institute of Dental Sciences, Nitte University, Deralakatte, Mangalore Gopakumar R Nair , MAHE Institute of Dental Sciences and Hospital, Chalakkara, Pallor, Mahe, India Subhas G Babu , Department of Dentistry and Radiology, AB Shetty Memorial Institute of Dental Sciences, Nitte University, Deralakatte, Mangalore
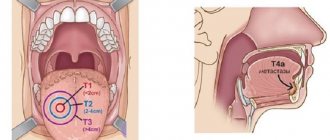
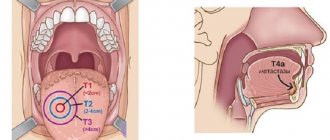
Symptoms of cheek cancer
Cheek cancer in the initial stages of the tumor process is asymptomatic. Any ulcer that is not prone to rapid healing and any area of hyperkeratosis should be regarded as an early stage of cancer. In the early stages of cheek malignancy, there is little or no pain. As the size of the cancer tumor increases, the following symptoms appear:
- Pain;
- Induration and infiltration of underlying tissues;
- Enlargement of regional lymph nodes, including damage to the lymph nodes of the submandibular triangle, jugular-digastric group and deep cervical lymph nodes.
What does cheek cancer look like? Any non-healing oral mucosal ulcer should be assessed as a potentially malignant tumor and consultation with an oncologist should be sought.
Do bumps on your gums hurt?
Painful sensations due to gum disease do not always occur. Often such pathologies are asymptomatic, which leads to delays in visiting the dentist and the occurrence of complications.
In non-infectious processes, swelling and formation on the gums are predominantly not accompanied by localized pain. The sensations may be general. So, if the jaw is injured, the entire area of impact may hurt. A cancerous tumor generally manifests itself as pain only after the beginning of the 2nd and subsequent stages. Teething can be painful, but when it comes to baby teeth, permanent teeth cause only minor discomfort in most cases.
Severe pain is characteristic of periostitis, which occurs as a complication of inflammatory processes affecting the periosteum and jawbone. With gingivitis and periodontitis, moderate pain may occur with mechanical and thermal effects, as well as with pressure. Pain with exostosis and epulis is felt with mechanical damage to the seal or the concomitant development of inflammation.
Despite the fact that periodontitis is an infectious process in which suppuration of tissue occurs, pain is not felt, especially in the presence of a fistula through which pus comes out.
As a rule, patients are driven to visit the dentist by pain. If they are absent, even if a lump is detected on the gum, going to the dentist is postponed. Such negligence often becomes a fatal mistake, since the period in which the tooth could be saved is missed. In addition to tooth extraction, a complication may be the spread of inflammation and abscess to healthy gum tissue and teeth.
Diagnosis of cheek cancer
If a tumor of the mucous membrane of the cheek is suspected, oncologists at the Yusupov Hospital conduct an examination using a mirror, palpation of the tumor and lymph nodes. If a long-term non-healing ulcer is detected, a biopsy is performed. If a negative result of histological examination of the material obtained during the biopsy is obtained, the suspicion of the malignant nature of the tumor remains, the biopsy is performed again.
Oncologists clarify the stage of the tumor process, assess the extent of spread of the malignant tumor from the buccal mucosa to adjacent tissues, and find out whether there are metastases to regional lymph nodes and distant organs. If the presence of metastases is suspected, computer and magnetic resonance imaging, ultrasound, and scintigraphy are used. Distant metastases are found in 20% of patients at the time of diagnosis.
Computed tomography and magnetic resonance imaging make it possible to assess the condition of the deeper anatomical structures of the oropharynx and surrounding tissues. If there is a suspicion of metastases to the lymph nodes or tumor infiltration of the floor of the mouth, a cytological examination of the aspirate obtained under ultrasound guidance is performed. To exclude distant metastases, a chest x-ray in two projections and an ultrasound examination of the abdominal organs are done.
Considering that the prognosis for cheek cancer is serious, a tomography of the neck, chest and upper abdominal cavity is performed. Using bone scintigraphy, I exclude bone metastases. Positron emission tomography allows one to identify the source of metastases in cases of undetected primary tumors.
A lump on the gum after dentures - is it dangerous or not?
A crown or denture is a common cause of gum swelling. A lump can occur both at the stage of preparation for the installation of a prosthesis, and some time after wearing artificial teeth.
If swelling occurs before the installation of dentures, the reason may be a violation of the depulpation procedure or poor-quality filling of the canals. Penetration of infection into the pulp provokes an inflammatory process that occurs in periodontitis.
Most often, after prosthetics, bumps appear on the gums due to poor quality of the prosthesis, discrepancy in the size of the crowns and errors when installing artificial teeth. The mucous membrane can be injured by the prosthesis. Even through small wounds, an infection penetrates, which leads to inflammation, or under constant exposure, a disruption occurs in the cells of the gum tissue, which begin to pathologically increase, forming a growth.
Treatment for cheek cancer
Malignant tumors are successfully cured using radical radiation therapy while preserving the function of the oral cavity. Radiologists implant radiation sources because it is possible to irradiate a small volume of tissue at a high dose. Radioactive isotopes of cesium, gold, radium, iridium, tantalum, which have the same efficiency, are used as sources.
For small tumors, the size of which does not exceed 1 cm, they are limited to implantation of a radiation source, without resorting to additional external influence. In cases of slightly larger tumors that are not suitable in size for implantation, external irradiation is used along with source implantation.
Traditionally, large cheek tumors are treated with external beam radiation. Recently, oncologists have been using a combination of radiation and chemotherapy. Mobile lymph nodes are radically excised. During prophylactic removal of lymph nodes without signs of damage, in a significant number of cases, foci of micrometastasis are found in them. For this reason, radiologists prefer to perform prophylactic irradiation of the neck in patients without evidence of lymph node involvement by the external beam, sometimes in combination with surgical treatment.
After surgery for cheek cancer, a cosmetic defect is formed. The results of surgical intervention are improved using the technique of microvascular free skin grafting. If a patient develops dry mouth after radiation therapy, he is prescribed oral pilocarpine. The drug increases salivation, which is usually accompanied by minor side effects - sweating and increased urination. For primary or secondary treatment of tumors of the buccal mucosa, patients are prescribed chemotherapy drugs.
Early diagnosis of a cheek tumor allows for effective treatment. If the tumor process is at a late stage, the prognosis worsens. If you experience unpleasant sensations in the oral cavity or identify ulcers of the buccal mucosa, undergo an examination at the clinic by calling the Yusupov Hospital.
Provoking factors
When a lump appears on the gum, it is important to correctly determine the underlying cause of the formation. In most cases, this is an exacerbation of an infectious disease that has already progressed in the patient.
A lump on the gum may be a consequence of:
- periostitis - manifests itself in the form of a fistula, which arose as an “exit” of pus accumulated in the area of the periosteum;
- periodontitis - purulent accumulation in the periodontium due to bacterial inflammation;
- cyst and granuloma are a consequence of periodontal abscess in the area of the tooth root, with the transition of purulent lesions to the mucous membrane;
- gingivitis is an inflammatory process in periodontal tissues with the formation of a non-purulent compaction.
A tumor in the form of a lump on the gums of teeth occurs due to non-infectious processes:
- teething - swelling of the gums in the form of a lump may be a sign of “advancement” of the tooth;
- fibroma - proliferation of connective tissue with the formation of a benign tumor;
- epulis - a growth that forms on the gum when pressure is placed on the gum due to teething pathologies, malocclusions, injuries and, in rare cases, hormonal imbalances;
- exostosis - the lump has a bone structure and is formed due to abnormalities of the jaw bone;
- hematoma - the formation is a “bag” of blood that has accumulated in a localized area of the mucosa after severe trauma.
If you consult a dentist in a timely manner, all pathological processes are eliminated using conservative or surgical treatment without consequences. A lump on the gum tissue poses a serious danger when gum cancer develops. Malignant disease is extremely rare and, apart from a lump in the area of the tooth root, there may be no symptoms.
Types of diseases with painful bumps
Treatment may include surgical removal of the lump, opening and removal of pus, medication, treatment of a deep problem (dental caries, gum disease).
Next, we will briefly look at the types of diseases with painful lumps. Remember that only a doctor can make a diagnosis. There is no need to try to determine the nature of the neoplasm yourself. There is also no need to intimidate yourself with possible complications - just sign up for a consultation and find out what treatment is necessary in your case.
- Hematoma. When a tooth erupts or after a mechanical injury, a bruise occurs. Most often it goes away over time, but sometimes the hematoma needs to be removed surgically to avoid inflammation of the gums.
- Fistula. If the root of a tooth is affected by caries, pus appears in the root canal and a tubercle appears on the gum. The tooth needs to be treated.
- Periodontitis, gingivitis. Inflammation of the gum tissue around a tooth affected by caries or due to mechanical trauma, poor hygiene - all this can cause formations to appear on the surface of the gum.
- Periostitis. Inflammation of the periosteum appears after a long inflammatory process in the tooth. This is possible after treatment of caries on a filled tooth.
There are other diagnoses that include various types of benign tumors and malignant neoplasms. In any case, be sure to contact your dentist!